
Ramsay Hunt Syndrome. A Case Report
Abstract
This case report describes facial nerve palsy due to Ramsay Hunt syndrome, highlighting otic vesicles, audiovestibular symptoms, and imaging considerations. Management with antivirals, corticosteroids, and supportive care is summarized. Early recognition can improve outcomes and limit sequelae.
Author Contributions
Academic Editor: Palaniappan Ramasamy, Director-Research, Sree Balaji Medical College and Hospital, Chennai, Tamilnadu, India.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2020 Nicolau Chafick Miguel Júnior, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction
As an human alpha herpes vírus, Varicella zoster virus (VZV), causes both varicella and varicella zoster. After a incubation period of approximately 2 weeks, viral replication starts in upper respiratory mucosa and after to skin vesicular rash. Latent infection occurs through viral access to the axons of sensory and ganglion neurons and also by axonal transport. During VZV reactivation period, vesicular eruption appears in neural path dermatome. Reactivation of VZV is most commonly found in immunodepressed patients, although, it can also be found in healthy individuals.
Ramsay Hunt syndrome, also named as herpes zoster oticus, is a rare condition that occurs due to (VZV) reactivation in the geniculate ganglion of the facial nerve.and in the vestibulocochlear nerve, causing sensorineural hearing loss and facial paralysis.1, 2, 3, 4, 5 In the present case report an unusual presentation of varicella zoster in an immunocompetent patient is reported.
Methods
The report of this case was submitted and approved by Universidade Metropolitana de Santos ethics committee. The patient was evaluated in a private medical clinic, as well as, complementary exams were performed in private laboratories.
Case Presentation
The present case refers to a 41-year-old caucasian man with a sudden, holocranial, severe and continuous headache that lasted two days. Right after this period, the patient experienced burning pain and the appearance of vesicles throughout the right auricle. At this moment, he also noticed a decrease in auditory acuity and the presence of tinnitus in this same side associated with gait instability and decreased facial mimicry of the right side of the face. His medical history was unremarkable. He was referred for neurological evaluation at a private clinic. During neurological examination, right facial paralysis was found (House-Brackmann scale grade II).6
Otoscopic examination revealed vesicles on the right auricle. Rinne and Weber's tests showed sensorineural hearing loss; Gait instability and Romberg sign on the right side were also found. Hematological tests were normal except for the presence of positivity on serologic (VZV) DNA polymerase chain reaction. Brain Magnetic Resonance Imaging (MRI) was performed and it was normal. Clinical evaluation and tonal audiometry were performed in a private otorhinolaryngology clinic and showed sensorineural loss on the right auricle. Cerebrospinal fluid analyses was not performed after the main diagnosis of Ramsay Hunt Syndrome was postulated. After clinical diagnosis, prednisone and valacyclovir were introduced for seven days with satisfactory results. The clinical evolution of the VZV treatment was satisfactory; It became evident during the treatment, the presence of mild right facial paralysis (House Brackmann scale grade II). (Figures A-E) Vertigo and postural instability treatment, as well as for tinnitus, were carried out with clonazepam and flunarizine and presented with sub-optimal response. Therapeutic follow-up with varicella zoster vaccine was proposed after 1 month of clinical treatment; Motor and vertigo rehabilitation were also instituted with partial results.
Figures A-E.Right Auricle varicella zoster vesicles. (A) Third day of clinical evolution (B) Seventh day of clinical evolution (C) Tenth day of clinical evolution (D) Fifteenth day of clinical evolution (E) Right facial nerve paralysis- House Brackmann scale grade II.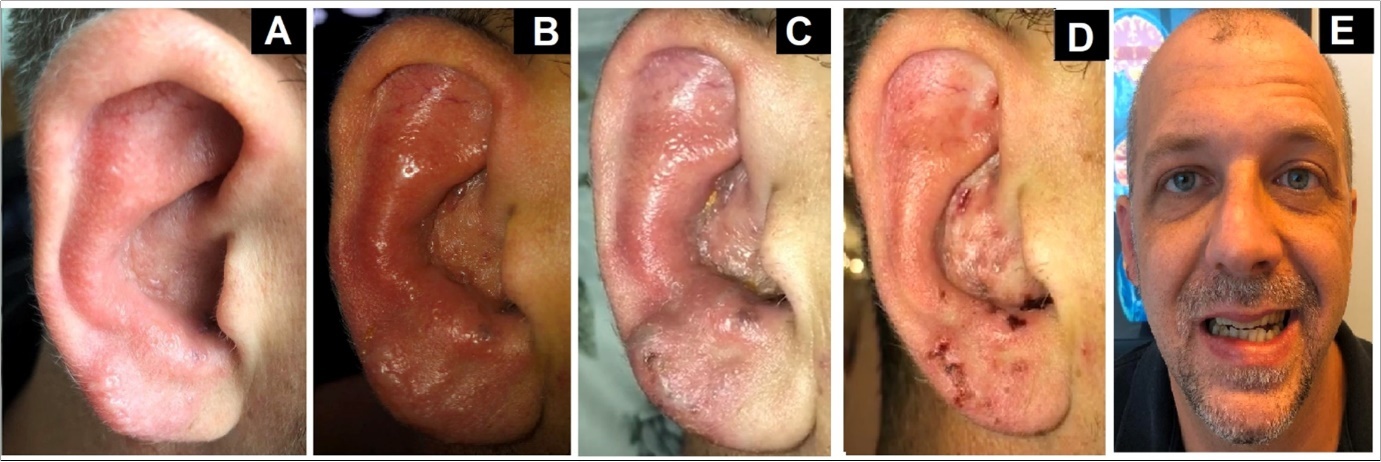
Discussion
Reactivation of VZV in the geniculate ganglion of the facial nerve and the vestibulocochlear nerve is a rare and uncommon condition in immunocompetent individuals.. Lumbar puncture and cerebrospinal fluid collection, although not mandatory for diagnosis, is specially recommended in cases of meningoencephalitis.7 The presente case, highlights Ramsay Hunt clinical evolution and treatment. Mild facial paralysis and vertigo presented incomplete remission and are in accordance with current literature.1, 2, 3, 4, 5
Conclusion
Ramsay Hunt syndrome is not an unusual VZV clinical manifestation and thus the case report confirms the findings described in current literature and shows vestibular and facial involvement. Attention to this clinical condition and evolution may help physicians make early and correct diagnosis.
References
- 1.Zerboni L, Sen N, Oliver S L. (2014) Molecular mechanisms of varicela zoster virus pathogenesis. , Nat Rev Microbiol; 12(3), 197-210.
- 2.Drone E, Ganti L. (2019) A Case of Disseminated Zoster in an Immunocompetent Patient. Cureus.;4;11(12): e6286
- 3.Pitton Rissardo J, Fornari Caprara AL. (2018) Herpes Zoster Oticus, Ophthalmicus, and Cutaneous Disseminated: Case Report and Literature Review. , Neuroophthalmology;27 43(6), 407-410.
- 4.ALC Paiva, JLV Araujo, Ferraz V R, JCE Veiga. (1992) Facial paralysis due to Ramsay Hunt syndrome - A rare condition. Rev Assoc Med Bras. 63(4), 301-302.
- 5.Sweeney C J, Gilden D H. (2001) Ramsay Hunt syndrome. , J Neurol Neurosurg Psychiatry 71(2), 149-54.
Cited by (1)
- 1.Amaravadi Divya, Parvathalu Reshma K., Ravinder Sunayana K., 2024, Ramsay hunt syndrome: a case report, International Journal of Scientific Reports, 10(11), 414, 10.18203/issn.2454-2156.IntJSciRep20243055