
Enduring Struggles and Protracted War: Hatred as a Multi-Faceted Construct
Abstract
This paper examines the concept of conflict- and war-related hatred as a multifaceted construct. Drawing upon various theoretical frameworks, we hypothesized that hatred in the context of conflict and war would encompass five distinct dimensions: Groupthink (Contagious Hatred), Destructiveness, Exposure, Chronicity, and Extreme-Severe Affect. To empirically validate this conceptual framework, we conducted a second-order factor analysis using data from 709 questionnaire responses collected from citizens in the Gaza Strip. The findings revealed that the optimal model comprises three primary constructs: Contagious Hatred, Chronicity, and Extreme- Severe Affect. Based on these results, we argue that collective existential threats in contexts of protracted conflict and war amplify groupthink, foster a sense of chronicity, and evoke intense negative affect. These findings underscore the complexity of hatred as a psychological and social phenomenon in conflict zones.
Author Contributions
Copyright © 2025 Izzeldin Abuelaish, et.al
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have no conflict of interest to declare.
Citation:
Introduction
The prevalence of hatred represents a critical public health and safety concern with far-reaching implications for individuals, communities, health systems, governments, and institutions both academic and non-academic. Hatred, defined as an intense and destructive attitude 1, manifests in various forms, including prejudice, bigotry, racism, fear, fearmongering, war, disease, violence, and cruelty 2, 3, 4, 5. These manifestations collectively undermine the health, welfare, and functionality of individuals and populations.
Although an expanding body of research highlights the detrimental effects of hatred on health, there remains a notable gap in the comprehensive study of hatred as a contagious phenomenon, a determinant of health, and a significant public health issue 2. Advancing our understanding of hatred and its associations with violence and adverse health outcomes is essential for developing preventive clinical interventions, therapeutic strategies, and informed social policies 2. Evidence- based initiatives rooted in such understanding can reduce violence rooted in hatred, mitigate its cascading health consequences, and address the global toll of conflicts, trauma, and deaths.
It is essential to recognize that contagious social and behavioral conditions often spread in patterns analogous to pathological illnesses, transferring from one individual to another through exposure. This phenomenon is evident in various domains, including violence 6, suicide 7, and organizational justice, where discussions of fairness can precipitate significant changes in attitudes and behaviors 8. Organizational network researchers have long studied social contagion, examining phenomena such as the alignment of moods 9, job satisfaction 10, organizational commitment 11, turnover intentions 12, and perceptions of job stress and work conditions within interpersonal networks 8. While these studies typically focus on relatively stable organizational contexts, the dynamics of social contagion in conflict settings are far more severe, often leading to widespread negative health outcomes, including violence.
This understanding parallels the transmission of viruses through populations. Pathological contagious diseases, such as COVID-19 and influenza, are well-documented examples of infectious illnesses 13. Similarly, social and behavioral contagions, including violence and hatred, follow predictable patterns of spread and can be anticipated, detected, prevented, and addressed through appropriate interventions.
To effectively address hatred as a contagious phenomenon, it must first be conceptualized and treated as a medicalized condition through public health and epidemiological frameworks. Like conventional diseases, hatred often originates from a causal agent or harmful exposure. Once exposure occurs, hatred may incubate within an individual, developing slowly through chronic, cumulative exposure or rapidly following acute exposure to a virulent and deleterious trigger. As this harmful exposure escalates, it adversely impacts the individual’s health and well-being. Depending on an individual’s tolerance and resilience, hatred may either propagate or be mitigated. If hatred proliferates, the affected individual may engage in actions that perpetuate hatred, resulting in trauma and the spread of hostility to others 14, 15.
By adopting a systematic and medicalized approach, public health initiatives can target the root causes and transmission pathways of hatred, offering novel opportunities to mitigate its effects and safeguard both individual and societal well-being.
Mechanisms of Contagion
Contagious diseases can spread quickly or slowly, depending on a host of factors and the virulence of the pathogenic agent. Virulence is the ability of the pathogenic agent to infect the host and cause the disease. For example, measles spreads quickly, whereas tuberculosis spreads slowly; gang wars and riots spread quickly, whereas other violence spreads much more slowly. For instance, victims of child abuse may become perpetrators of family violence many years later. In addition, on a biological level, as humans built to mimic one another, research involving monkeys have shown that we have certain types of neurons, called mirror neurons that fire when simply watching someone else carry out an action, even when we ourselves are not doing the same thing 16. This transmission of information is controlled by the premotor cortex system, which helps humans learn various behaviors by imitation - including violent behaviors. When we watch someone else behave violently, mirror neurons activate our own motor system as if we are doing the action ourselves 16, 17. Mirror neurons are suggested to be the missing link in explaining the biological mechanism of how violence spreads like infectious diseases and models the phenomenon of contagion as well defined and seen when one is infected by the flu 16.
Hatred: Where does hatred start? Do we have any role in the shaping of our biology or our neurology or our chemistry, what are the forces and factors that determine our behavior? According to theories of human behaviour, the behaviour of a human being is determined by four primary factors namely, biological factors such as age and sex, biosocial factors which refers to how people interact with each other, cultural factors, specifically the culture which one belongs to, and the situational factors, such as the environmental challenges one faces 18, 19.
Newton's third law in physics states: that for every action, there is an opposite reaction 20, 21. Much like Newton’s third law, we speculate that in relation to hatred, once provoked or exposed, an equal and opposing reaction or extreme opposite reaction occurs in response to that action, which manifests as a destructive, contagious disease in the form of hatred, as an emotional or physical response 2, 15. In addition, we need to consider that, although we are wired to respond to other people, there is also a tremendous amount of variability in individuals’ ability to transmit their emotions to others. Some research suggests, more outgoing, and expressive individuals tend to be better transmitters or be more successful at having you feel what they feel 22, 23.
Contagion appears to involve both biological and social processes. It is pervasive, and yet we are often unaware of the influence of other’s emotions and behaviors on our own. This is particularly striking because the consequences of contagious behavior can be significant’ 23. For example, mechanisms of contagion can occur through a phenomenon known as mass psychogenic illness, in which symptoms are passed from person to person among people who are visible to one another 24. ‘Mass psychogenic illness is an extreme example of the more general phenomenon of contagious behavior: the unconscious transmission of actions or emotions from one individual to another’ 23. Similarly, Hatfield, Cacioppo, & Rapson 22 define primitive emotional contagion as: The tendency to automatically mimic and synchronize facial expressions, vocalizations, postures, and movements with those of another person's and, consequently, to converge emotionally’ (p. 5). Glaeser 25 who analyzes the political economy of hatred, claims that hatred is fostered with stories about the crimes of the out-group (the other side). Yet, these stories are not based on truth. Politicians create hate-fulling stories in order to discredit opponents and create harm-based hatred.
Dr. Martin Luther King, Jr. noted in 1958 that “violence begets violence,” recognizing the contagious aspect of violence. More recently, there is hard science to back up King's observations. Indeed, violence is considered contagious and a public health issue 17, 26. We see violence causing violence in its most acute setting in cases of retaliations in gang violence 27 and even in war. For example, this was seen in what was called civil, or intrastate, wars, such as following the 2005 bombing of the Samarra Mosque in Iraq, or even what we call wars between states, or interstate wars, such as World War II 26.
Pathological and physical diseases are not the only diseases that are communicable and contagious. Social, mental, emotional processes and behaviors are socially contagious and can spread from one person to another. Some self-destructive teen behaviors, in fact, are extremely socially virulent and can spread among groups as rapidly and destructively as a physically contagious disease. For example, among teens, the results from one study showed that violence can spread up to four degrees of separation 28. Youth violence is a particularly serious problem everywhere, but especially in the U.S. According to David-Ferdon & Simon 29, in the U.S., more youth die from homicide each year than from cancer, heart disease, birth defects, flu and pneumonia, respiratory diseases, stroke, and diabetes combined. Youth homicide rates in the U.S. are three to 40 times higher than rates in similarly high-income countries 29, 30. In lieu of these findings, it is important to consider the virulent factors that increase the risk of exposure and contagion, such as the contextual aspects, the environment, policies (e.g., gun policies), discrimination, and history that is inherently embedded within the root of our existence.
Given that hatred is a contagious disease and public health issue, then disease is an impairment of the normal state (functionality) of the person or one of its parts that interrupts or modifies the performance of vital functions. Disease is a pathological process, most often physical, sometimes undetermined in origin 31, and it is a disease of the mind 32. Hatred is also a disease of the human heart, soul, and body Hatred is a complex process that attacks humankind and becomes a community disease. In addition, Hatred is a complex state, discrete, involves destructive intent, is contagious to individuals, groups and communities and is often the result of exposure to harm 1, 14, 15. Abuelaish 15 argues that “A disease is an impairment of an organism caused by external or internal elements that are harmful to that organism and is recognizable by its symptoms. Hatred is a disease. Such a conceptual framework is based on the interplay of exposure, human hosts, and the environment that leads to the production of hatred” 15 p.60
Conceptualizing Hatred as a disease requires a valid scientific medical model to investigate the causes, characteristics, and impact of hatred on health and well-being using a multidisciplinary comprehensive and holistic approach rather than a fragmented one. A multisystem approach is needed to include socio-biomedical, psychological, sociological, psychiatric, neurological, and endocrine variables. Hatred is an overlooked epidemic and contagious disease 14.
Biopsychosocial Model and Public Health Approach
It is assumed in Engel’s biopsychosocial model that disease or illness outcome is attributed to the intricate blend of biological, psychological, environmental, and social factors described in systems hierarchy from molecules to the universe with the patient at the central interfaces in the hierarchy 33. This model is perceived to be still valuable and important 34, 35.
The model is also relevant to the concept of hatred as a contagious disease, from a multitude of angles which provides a multidisciplinary approach. Specifically, one which offers a comprehensive, holistic, biomedical model to study the patho-physiology of hatred. This model helps to acknowledge the social, economic, political, environmental, and cultural factors which influence the spread of hatred as a contagious disease, as it is contextual based and depends on who you are and where you are.
Hatred is a public health issue because hatred often engenders violence, sometimes affecting entire populations. Nevertheless, direct, and indirect data suggests that hatred is a public health issue also because of its association (causal, correlated, or otherwise) with several other usually stress-related health problems. Furthermore, hatred itself is disease-like, being caused or triggered by exposure to harmful environmental variables and presenting attributes such as malignancy and contagiousness.
Causal Relationship and the Epidemiological Triad (Exposure)
From the literature, it is speculated that the disease of hatred stems from specific or cumulative triggers 36. In our research, we show how hatred is a contagious disease. Using the epidemiological triad (Figure 1), this idea can be further explained 37. This proposed model involves the agent, host, and environment or context. The agent is the necessary factor leading to disease onset (e.g., the harm that can lead to the onset of the disease). The host is the individual or group who is susceptible to the agent. Then the environment is a set of factors that combine with the agent contributing to disease onset. Using hatred in this model, the agent can be identified as a causal trigger or agent to hatred. Examples of the causal agent and triggers include racism, discrimination, violence, hate speech, hate crime, misinformation, fear mongering, bigotry, oppression, and aggression 14, 15. The host would be individuals who are direct targets of hatred or people who are indirectly exposed to hatred through their environment or media.
We speculate that triggers of specific cases of hatred are likely to be cumulative exposures to repetitive harm, often violent or provocative (physical, psychological, social, political, including deprivation and dehumanization), stimulation. Hatred is interconnected with the triggers as the effect is bidirectional. Hatred causes responses in the person with hatred. These responses include racism, discrimination, violence, etc. Therefore, the response is the same as the initial trigger to hatred, hence, its bidirectionality and interconnected nature 2. However, it is unclear how these triggers lead to hatred instead of other emotional responses, as well as hatred’s means of transmission and its infectivity. There may be a causal relationship between exposure to these triggers and hatred as an outcome, warranting further exploration from a public health perspective 15. Specifically, a public health approach to hatred is needed in investigating its pathophysiology and socio-epidemiology, identifying modifiable risk factors, prevention, and management strategies, and how to predict early detection for early prevention.
Figure 1.Epidemiological Triad of Hatred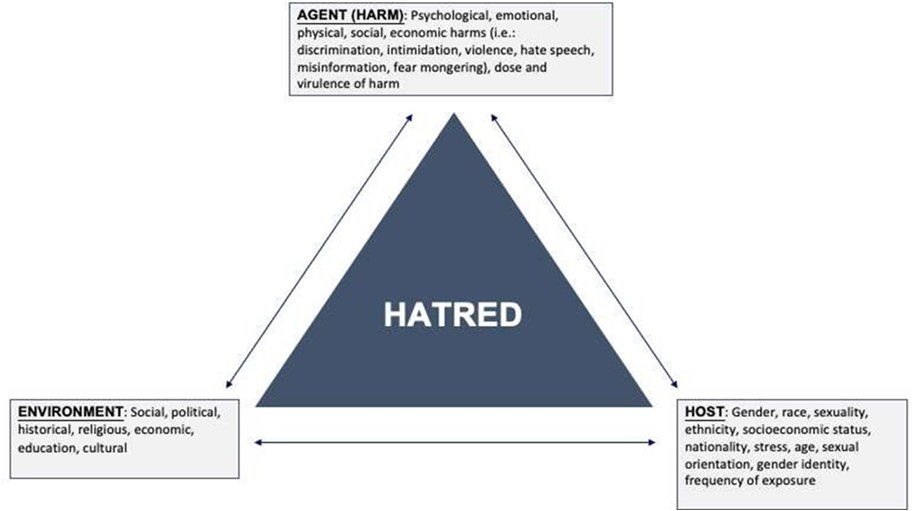
Figure 1 presents a model in which Violence/War Related Hatred is associated with a triangular interrelation between the specific characteristics of the individual, the individual experience of harm and the environment in which the individual lives and that has an impact on his emotions. Based on the proposed model, we claim that hatred, while often conceptualized as an extreme form of anger, is an infectious and contagious manmade disease. It is a result of exposure to painful, and deleterious harm attributed to the intricate relationship between contextual, biological, psychological, and social factors and occurs in clusters. We therefore created the five main dimensions of Conflict/War Related Hatred including Group Think, Destructive, Exposure, Chronicity, and Strong Affect (Extreme-Severe). Next, we check their reliability base don the inter-correlations between the variables in each dimension. Finally, we aim to analyze the interrelations between the five dimensions of hatred in order to examine whether they create one unified and valid construct of Conflict/War Related Hatred.
Based on the above theoretical review, the main research questions that are the focus of this paper are: what the dimensions of conflict/war related hatred are; how they are related to each other, and whether they form a combined unified reliable statistical construct. In the Method section below, we present our data collection process in the Gaza Strip, the main demographic variables of the sample, and the five empirical dimensions of our theoretical model. Then we conduct a Second Order Factor Analysis to confirm or disconfirm the interrelations between the five dimensions that lead us to the final Hatred construct that is based on only three reliable and valid dimensions out of the five dimensions in the original model.
Methodology
Study Design and Setting
The first step was obtaining and ethics approval for the study. Ethics approval from the University of Toronto Research Ethics Board (protocol ID: 37953) was obtained.
The study is cross-sectional and is stratified random sample. The first step was a geographic ratification of the major neighborhoods in the five main cities in the Gaza Strip. Once the five strata were defined, a random sample within each cluster was selected. The data were collected through a community-based face to face survey on the topic of “Developing a Measure of Hatred and its Impact on Health and Wellbeing”, designed and developed by the first author. Then the data were coded, digitized, checked and cleaned by the research team.
Hatred Model Dimensions
Based on the proposed model, we started with a definition of hatred that is based on 122 items (with a 5 points Likert scale), composed by 5 dimensions operationalized as latent constructs: Group Think, Destructive, Exposure, Chronicity and Strong Affect where each of the latent constructs can be measured by specific items and the full model explored and tested as a second order factor model.
1. Contagious/Group Think- One of the components of hatred is group think, defined as an in-group spread of negative ideas about an out-group. Individuals with high level of hatred have a necessity to share their emotional state with others which will give hatred a dynamic similar to that of a traditional contagious disease. 14 items were used to measure this dimension.
2. Destructiveness– Hatred often includes a desire to eliminate /destroy/ control the target of hate physically, psychologically, and/or socially; this often involves a compromise in moral judgement, including self-righteous cruelty and/or lack of remorse. 36 items were used to measure this dimension.
3. Exposure- Hatred often involves distortions in memory, perception, and judgement such as: vulnerability to distorted historical accounts, propaganda, and charismatic leaders; attributions of unrealistic power and importance to the hatred object; evaluation of the objects as bad (dangerous, immoral, inhuman) degrading/devaluing the object as subhuman. 17 items were used to measure this dimension.
4. Chronicity – characteristics are chronic and sometimes obsessive. 16 items were used to measure this dimension.
5. Strong Affect (Extreme-Severe) contains strong, intense affect. 51 items were used to measure this dimension.
Scale Development
Hatred Multi- Construct Validity and Reliability
Based on related literature on different dimensions of Conflict/War Related Hatred, the questionnaire included 122 items that aimed to measure the multi-construct measurement of hatred. The initial non-statistical validity and reliability tests of the items were based on several steps.
First, five experts in the field of hatred research were asked to classify the 62 items in the questionnaire that were related to the hatred theoretical construct presented above. The items that were classified in the same construct category by at least 3 out of the 5 judges were considered to be adequate to demonstrate reasonable consensual face and content validation. The results of this step, 45 out of the 62 items received high consensus among the judges, based on face and content validity.
Next, the five original constructs of the model were examined for the level of inter-judge reliability. Then, we conducted tests of face validity and content validity by three independent (non-experts) examiners. They examined the degree to which the items seemed to constantly belong to the same content construct by the theoretical definition we used.
Statistical Analysis
Initial descriptive analysis was conducted to evaluate data integrity. Means, standard deviation and proportion of agreement were calculated for each item. Reliability analysis was conducted in SPSS, where Cronbach’s alpha, inter-item correlation, item-total correlation, and Cronbach’s alpha if item was deleted were all calculated and used for a first re-specification of the structure of the 5 constructs. Items were removed if they caused Cronbach’a alpha to increase when removed from the construct and/or if they had a correlation with the total construct score less than 0.30. The total construct score was calculated with the item removed, then a correlation is calculated between this total score and the item. This was done for each and every item in each of the five constructs.
The Hatred Factor dimensions
In order to test our theory about the theoretical constructs of hatred, we adjusted a second order factor analysis using software Mplus. The five constructs described above were specified as latent variables following a confirmatory factor analysis structure, where each construct loaded into a single factor: the Hatred Factor. Each of the 5 latent factors were in their turn measured by specific pre-defined observed items that loaded on them. The resulting Second Order Factor model was estimated via full maximum likelihood estimator (FMLE) with robust standard errors 38, 39. The resulting Second Order Factor model was estimated via full maximum likelihood estimator (FMLE) with robust standard error 38, 39. The FMLE uses all available data so that subjects with missing values are not dropped out of the data used by the model. The model was evaluated based on fit CFI (Comparative Fit Index), TLI (Tucker-Lewis index), RMSEA (Root Means Square Error of Approximation), SRMR (Standardized Root Mean Square Residual) and BIC (Bayesian Information Criteria) 40, estimated value of standardized loadings and modification indices. The only re-specification of the model was the removal of dimensions that did not load significantly on hatred.
Results
The Main Demographic Variables of the Sample
The sample contains 709 subjects that live in the five main cities of the Gaza Strip. The demographic variables of the sample and their distributions are presented in Table 1. The main demographic characteristics are: 47% males and 53% females, the average age was 29.8 with a range of 15 to 71 years. Most respondents were married (48.9%) or single (40.9%) and 50.5% had children. The level of education was relatively high and 47.8% had a university education with a BA degree. For more demographic variables, please see Table 1.
Table 1. The Main Demographic Variables of the Sample| # Of | |||
| Gender | Children | ||
| 1. Male | 333 (47.0) | 0 | 2 (0.3) |
| 2. Female | 374 (52.8) | 1 | 65 (9.2) |
| Missing values | 2 (0.3) | 2 | 74 (10.4) |
| 3 | 60 (8.5) | ||
| Age | 4 | 62 (8.7) | |
| 1. 15 to 25 | 272 (38.4) | 5 | 39 (5.5) |
| 2. 26 to 45 | 363 (51.2) | 6 | 19 (2.7) |
| 3. 46 to 71 | 56 (7.9) | 7 | 17 (2.4) |
| Missing values. | 18 (2.5) | 8 | 10 (1.4) |
| 9 | 9 (1.3) | ||
| Mean SD = 29.80 0.50 | 10 | 2 (0.3) | |
| Median = 28.0 | 13 | 1 (0.1) | |
| Missing | |||
| Mode = 30 | values | 349 (49.2) | |
| Range = 15 - 71 | |||
| Mean | |||
| SD= | |||
| 3.51 | |||
| 2.17 | |||
| Median - | |||
| Marital Status | 3.0 | ||
| Mode- | |||
| 1. Single | 290 (40.9) | 2 | |
| Range - 0 | |||
| 2. Divorced | 28 (3.9) | - 13 | |
| 3. Married | 347 (48.9) | ||
| Main | |||
| areas and | |||
| 4. Widowed | 23 (3.2) | Cities | |
| Missing values | 21 (3.0) | 1. Rafah | 123 (17.3) |
| 2. Khan | |||
| Younis | 131 (18.5) | ||
| 3. Middle | |||
| Level of Education | Area | 121 (17.1) | |
| 1. Primary & Middle School | 39 (5.5) | 4. North | 233 (32.9) |
| 2. High School | 155 (21.9) | 5. Gaza | 100 (14.1) |
| Missing | |||
| 3. College | 107 (15.1) | values. | 1 (0.1) |
| 4. University - BA | 339 (47.8) | ||
| 5. University - MA & PhD | 21 (3.0) | Member | |
| Missing values. | 48 (6.8) | of | |
| Political | |||
| Party | |||
| Having Children | 1. Yes | 178 (25.1) | |
| 1. Yes | 358 (50.5) | 2. No | 478 (67.4) |
| 2. No | 289 (40.8) | Missing values | 53 (7.5) |
| Missing values | 62 (8.7) | ||
| Live in a Safe / Peaceful Area | |||
| 1. Yes | 293 (41.3) | ||
| 2. No | 366 (51.6) | ||
| Missing values | 50 (7.1) | ||
Reliability Analysis
The initial model, as defined by expert input, is shown in Figure 1. Table 2 shows all items in each of the three dimensions and presents the Reliability analysis of each of the five the three final dimensions of Conflict/War Related Hatred
Table 2. Cronbach Reliability Analysis of the five Hatred Dimensions| Items within Dimensions | Mean | Std.Deviation | Corrected Item-Total Correlation | Cronbach's Alpha if ItemDeleted | Estimate | Std. Error | Est. / S.E. | P-Value |
| Group Think (Contagious) Items | ||||||||
| H5. I believe we need to tell our children about atrocities and threats we were exposed to by other groups of people. | 3.27 | 1.412 | 0.304 | 0.728 | 0.34 | 0.04 | 8.5 | <.001 |
| H21. The public should be informed about the danger of certain groups. | 3.62 | 1.272 | 0.434 | 0.702 | 0.53 | 0.03 | 16.3 | <.001 |
| H33. We need to teach our children about the danger of certain groups of people. | 3.68 | 1.275 | 0.460 | 0.697 | 0.55 | 0.03 | 16.2 | <.001 |
| H56. Members of my community talk about how to defeat the evil of some groups of people. | 3.32 | 1.147 | 0.415 | 0.706 | 0.48 | 0.04 | 12.6 | <.001 |
| H57. I expect my family, friends and group to share my views. | 3.32 | 1.148 | 0.333 | 0.719 | 0.37 | 0.04 | 9.0 | <.001 |
| H81. I tell my family members not to trust certain groups of people. | 3.34 | 1.247 | 0.365 | 0.714 | 0.46 | 0.04 | 12.4 | <.001 |
| H98. I warn my friends and family about the dangers of certain groups of people. | 3.61 | 1.168 | 0.546 | 0.684 | 0.61 | 0.03 | 20.1 | <.001 |
| H102. People need to take an active role speaking out against certain groups of people. | 3.27 | 1.261 | 0.366 | 0.714 | 0.43 | 0.04 | 11.2 | <.001 |
| H109. My friends and I talk about the danger of certain groups of people. | 3.26 | 1.239 | 0.454 | 0.699 | 0.57 | 0.03 | 17.2 | <.001 |
| Sub-Scale - Group Think / Contagious: - Mean = 30.71; Standard Deviation = 39.75; # of items = 9; n = 644; Cronbach's α = .73. | ||||||||
| Chronicity Items | ||||||||
|---|---|---|---|---|---|---|---|---|
| H35. I have disliked a certain group of people for many years. | 3.22 | 1.359 | 0.301 | 0.678 | 0.45 | 0.05 | 10.2 | <.001 |
| H66. Every day I think about a group of people that I dislike. | 2.39 | 1.274 | 0.419 | 0.650 | 0.49 | 0.04 | 11.8 | <.001 |
| H 69. I cannot stop myself from thinking about certain groups. | 2.67 | 1.249 | 0.428 | 0.649 | 0.54 | 0.04 | 14.5 | <.001 |
| H80. I often blame others for adversities in my life. | 2.74 | 1.340 | 0.358 | 0.664 | 0.42 | 0.04 | 10.3 | <.001 |
| H86. There is a group of people I dislike that is always on my mind. | 2.49 | 1.254 | 0.440 | 0.646 | 0.52 | 0.04 | 12.7 | <.001 |
| H90. I sometimes cannot get the threat of certain groups of people out of my mind. | 2.69 | 1.323 | 0.382 | 0.659 | 0.48 | 0.04 | 13.3 | <.001 |
| H108. I cannot forgive the people who threatened me or did me harm. | 3.00 | 1.335 | 0.338 | 0.669 | 0.46 | 0.04 | 10.6 | <.001 |
| H113. I feel distracted a lot. | 3.04 | 1.298 | 0.372 | 0.661 | 0.46 | 0.04 | 11.4 | <.001 |
| Sub-Scale - Chronicity: - Mean = 22.24; Standard Deviation = 5.85; # of items = 8; n = 661; Cronbach's α = .69. | ||||||||
| Strong Affect (Extreme-Severe) Items | ||||||||
| H10. There is agroup of people that you can never trust. | 3.95 | 1.291 | 0.367 | 0.806 | 0.43 | 0.04 | 11.000 | <.001 |
| H14. Certain groups of people have been proven to be liars. | 4.02 | 1.266 | 0.471 | 0.798 | 0.55 | 0.04 | 15.400 | <.001 |
| H15. A certain group of people is repugnant to me. | 3.58 | 1.266 | 0.568 | 0.791 | 0.62 | 0.03 | 19.200 | <.001 |
| H23. There are groups of people that can destroy our normal way of living. | 3.67 | 1.254 | 0.503 | 0.796 | 0.56 | 0.03 | 16.300 | <.001 |
| H31. Some groups of people are loathsome to me. | 3.25 | 1.315 | 0.574 | 0.790 | 0.60 | 0.03 | 19.400 | <.001 |
| H37. I feel compelled to speak out against certain group of people. | 2.65 | 1.301 | 0.234 | 0.816 | 0.30 | 0.04 | 7.600 | <.001 |
| H40. Some people cannot atone for their sins. | 3.18 | 1.297 | 0.373 | 0.806 | 0.44 | 0.04 | 12.400 | <.001 |
| H 45. I feel that there are certain groups of people I cannot trust at all. | 3.65 | 1.274 | 0.524 | 0.794 | 0.56 | 0.03 | 17.600 | <.001 |
| H48. People in certain groups deserve to be punished. | 3.75 | 1.244 | 0.480 | 0.798 | 0.53 | 0.03 | 15.600 | <.001 |
| H55. I know that certain groups are plotting to destroy us. | 3.47 | 1.311 | 0.507 | 0.795 | 0.57 | 0.03 | 18.300 | <.001 |
| H65. If we do not act, certain groups of people will make it impossible for us toexist. | 3.46 | 1.304 | 0.449 | 0.800 | 0.48 | 0.04 | 12.700 | <.001 |
| H83. People in some groups deserve to die. | 2.89 | 1.374 | 0.324 | 0.810 | 0.34 | 0.04 | 8.800 | <.001 |
| H89. We must never waver in our fight against certain groups of people. | 3.21 | 1.359 | 0.376 | 0.806 | 0.45 | 0.04 | 12.400 | <.001 |
| H94. There is a group that abuses others all the time. | 3.55 | 1.299 | 0.376 | 0.805 | 0.48 | 0.04 | 13.300 | <.001 |
| Sub-Scale - Extreme-Severe / Strong Affect:- Mean = 48.28; Standard Deviation = 9.80; of items = 14; n = 600; Cronbach's α =.81. | ||||||||
Group Think/Contagious Dimension: Includes 9 items out of the initial 14 items. For all these items, the Cronbach's Alpha if Item Deleted is lower than the final Cronbach’s Alpha that has the value of .73, and therefore these 9 items were included, while the other 5 were excluded.
Destructiveness: Destructiveness is the capacity or tendency to do damage to oneself, other people or beings, or non-living objects. Since harm happens all the time out in the world, I would argue that almost everything in the world contains some element of destructiveness. For example, even a parent’s love for their child, which we might consider the most beautiful thing in the world, becomes destructive when it means lying to the police about a child’s behavior or enabling a child to continue pursuing their drug addiction. People can be exposed to various forms of destructiveness: cultural destructiveness 41, Destructive Leaders 42.
Destructiveness in the context of social pathological disease (Hatred) refers to the capacity of these conditions to cause significant harm to individuals, communities, and societal structures. This harm manifests in various forms, including psychological distress, economic losses, and the breakdown of social order. Social pathologies are characterized by behaviors and conditions that not only deviate from societal norms but also actively deteriorate the well-being of society 43.
Hatred detrimentally affects the health, wellbeing, functionality and social structure of individuals and communities. The exposure to these social pathological agents, unlike medical biological, are rooted in social, economic, and cultural dysfunctions. Therefore, hatred as a contagious disease reflects deeper societal dysfunctions that require comprehensive and collaborative approaches for resolution. Addressing these issues involves economic, educational, and social interventions aimed at creating a more equitable and cohesive society. Understanding the multifaceted nature of this destructiveness is crucial for developing effective interventions and creating a more resilient and cohesive society.
Exposurerefers to the contact or proximity of individuals or populations with factors that can influence health outcomes. These factors can include a subject's attributes (association) or agents (effect), such as biological, chemical, social, ecological, psychological, or physical elements, which may impact their health 44. Exposure encompasses contact over time and space, making it a broad concept that includes short-term (acute), intermediate, or long-term (chronic) contact with these agents.
The effects of exposure are influenced by several factors, including the individual's susceptibility, the virulence and intensity of the agent, and the frequency and duration of contact. Additionally, geographic factors, the time frame, and the nature of exposure (continuous, persistent, cumulative, or intermittent) also play a crucial role. Therefore, measuring exposure involves assessing these elements to understand their potential health effects and identifying how people come into contact with hazardous substances or are exposed to harm 45.
Understanding exposure is crucial in epidemiological research for identifying risk factors, establishing causality, and designing interventions. Further, this concept is integral to understanding the distribution and determinants of health within populations. Accurate assessment and mitigation of exposure are vital for improving public health and reducing disease burden.
Chronicity Dimension: Includes 8 items out of the initial 16 items. For all these items, the Cronbach's Alpha if Item Deleted is lower than the final Cronbach’s Alpha that has the value of.69, and therefore these 9 items were included, while the other 7 were excluded.
Strong Affect (Extreme-Severe) Dimension: Includes 14 items. For all these items, the Cronbach's Alpha if Item Deleted is lower than the final Cronbach’s Alpha that has the value of.73, and therefore these 9 items were included while the other 36 items were excluded.
Our initial second-order factor analysis model had the second-order factor Hatred loading on all the 5 first-order constructs. The model showed reasonable fit indices (RMSEA, SRMR, CFI and TLA were 0.052, 0.075, 0.70 and 0.69 respectively; Chi-square (1415) = 4163, p<0.0001), but the loading of the second-order factor Hatred on the first-order construct Destructive was not significant (loading < 0.001, SE = 0.12, p = 0.979), so that we decided to remove it from the model. Looking at model estimated correlations between the first-order factors, we noticed that Destructive had very low and non-significant correlation (no shared variance) with Group Think and Strong Affect, providing evidence that Destructive is not consistent with the definition of the role of the first-order factors, which are expected to be correlated since they are indicators of the same Hatred construct. The model was then re-specified with the remaining 4 first-order factors and this time we were not able to obtain estimates because of the low shared variance between Exposure and Chronicity, which caused Exposure to also be removed.
Our final model, which loadings of observed items are shown in Table 2, and loadings of the first order factors are shown in Table 3, kept three first-order factor showed improved fit indices (RMSEA = 0.052, SRMR = 0.06, CFI = 0.8 and TLI = 0.78, Chi-square (429) = 1263, p <0.0001).
Table 3. Second-order factor analysis for the three constructs of Hatred| Hatred (Second-order Factor) | Estimate | Standard. Error | Est. / S.E. | P- Value |
| Group Think | 0.380 | 0.067 | 5.688 | 0.000 |
| Chronicity | 0.787 | 0.029 | 26.784 | 0.000 |
| Strong Affect | 0.739 | 0.035 | 21.129 | 0.000 |
We argue that this model describes a reasonable hypothesized structure of the constructs involved in the definition of Hatred. As such, Hatred can be measured and quantified by the level of Chronicity, group Think (Contagious) and Strong Affect. The constructs of Exposure and Destructive as defined and operationalized, do not seem fit this Second Order Factor Structure, but could be part of a broader definition of Hatred, one that would include more heterogeneous sub-scales.
Discussion
Our research focuses on analyzing certain psychological constructs and their relationships. Our findings showed the relevant and related results between the three constructs: group think (contagious), chronicity, and strong affect (Extreme-Severe). We need to consider further research to find out the relation with each construct outcome variable to health measure and wellbeing.
The study started by considering five psychological constructs. Constructs are fundamental concepts that were used to represent specific aspects of human behavior, thoughts, or emotions. In our case, the five constructs being studied are:
1. Group Think (contagious): Groupthink is a psychological phenomenon where a group of individuals prioritizes consensus and conformity over critical thinking and independent decision-making. This can lead to poor decision-making and a lack of diverse perspectives within the group. The term "contagious" indicates that this behavior spreads within the group, implying that when one or a few members exhibit groupthink tendencies, it can influence others to adopt similar behaviors.
2. Chronicity: Chronicity refers to the persistent nature of certain behaviors or conditions over an extended period. In the context of group dynamics, chronicity might suggest that specific behaviors associated with groupthink or other constructs persist over time, shaping the overall culture and functioning of the group. For instance, if a group consistently displays groupthink behavior, it can become a recurring pattern in their decision-making processes.
3. Strong Affect (Extreme-Severe): The term "strong affect" refers to intense emotional responses experienced by group members. When these emotions are categorized as "Extreme-Severe," it suggests that the emotional reactions within the group are not just mild feelings but rather intense and potentially overwhelming emotions. Such strong emotions can significantly impact how group members interact, communicate, and make decisions.
The significance of the "relevant and related results" lies in the connections discovered between these three constructs:
1. Group Think (contagious) and Chronicity: The relationship between groupthink and chronicity suggests that when groupthink behaviors become entrenched over time, they can evolve into chronic patterns of conformity and limited critical thinking. This can hinder the group's ability to adapt to new challenges, stifling creativity and innovation.
2. Group Think (contagious) and Strong Affect (Extreme-Severe): The connection here implies that the strong emotions associated with extreme-severe affect can amplify the spread of groupthink behaviors. When individuals within the group experience intense emotions, they might be more susceptible to conformity, making it easier for groupthink to take hold and spread contagiously.
3. Chronicity and Strong Affect (Extreme-Severe): This relationship suggests that over time, chronic patterns of behavior can lead to heightened emotional responses. For example, if a group repeatedly engages in destructive behaviors, it could lead to strong negative emotions, intensifying the overall affect within the group.
In summary, the study's findings highlight the intricate relationships between groupthink (contagious), chronicity, and strong affect (Extreme-Severe). These constructs interact in ways that influence how groups function, make decisions, and experience emotions. The connections discovered in the study emphasize the importance of addressing these factors to promote healthier group dynamics, effective decision-making, and better emotional well-being within groups.
By conducting comprehensive research on the relationships between group dynamics constructs and health measures/wellbeing, organizations and leaders can better understand the potential risks and benefits of these dynamics. This knowledge can guide interventions and strategies aimed at creating healthier and more productive group environments. Remember to integrate existing theories and models and cite relevant sources to strengthen your elaboration.
We need to consider further research to find out the relation with each construct outcome variable to health measure and wellbeing.
The statement "We need to consider further research to find out the relation with each construct outcome variable to health measure and wellbeing" suggests the importance of conducting additional research to understand how the identified constructs (groupthink, chronicity, and strong affect) are connected to specific outcomes related to health measures and overall wellbeing. Here's a more detailed explanation of this concept:
Construct Outcome Variables
Groupthink (contagious): Research could investigate whether exposure to groupthink behaviors and the contagious spread of conformity within a group have any correlations with physiological and psychological health measures. For instance, does being part of a group characterized by groupthink tendencies contribute to increased stress levels, decreased job satisfaction, or higher rates of burnout among individuals?
Chronicity: Exploring the impact of chronicity in group dynamics on health and wellbeing involves understanding how persistent patterns of behavior affect individuals over time. Does chronic exposure to group dynamics marked by conformity lead to feelings of frustration, reduced self-esteem, or even physical health issues? Long-term experiences of chronicity might have cumulative effects on overall wellbeing.
Strong Affect (Extreme-Severe): Investigating the relationship between strong emotional affect and health outcomes is crucial. Does experiencing intense emotions within a group context contribute to mental health challenges, such as anxiety or emotional exhaustion? Are there physiological changes that can be linked to these emotional experiences?
Health Measures and Wellbeing
Health Measures: Further research should explore potential links between the identified constructs and objective health measures, such as blood pressure, heart rate variability, cortisol levels, and immune system function. Are there quantifiable physiological responses that can be associated with chronic exposure to groupthink, strong emotional affect, and other dynamics?
Wellbeing: Research should also delve into the impact of these constructs on overall wellbeing, encompassing psychological, emotional, and even physical aspects. Does being part of a group with chronic groupthink behaviors correlate with lower life satisfaction, a decreased sense of belonging, or even increased rates of absenteeism due to stress-related health issues?
Implications and Applications
The findings of this research can have implications for organizational policies, leadership strategies, and intervention programs. Understanding how group dynamics affect health and wellbeing can guide efforts to create more supportive and healthy work environments.
The results can also inform the development of targeted interventions that address specific challenges arising from these dynamics. For example, if strong affect is linked to reduced wellbeing, organizations can implement strategies to help individuals manage their emotions effectively.
In summary, further research is needed to comprehensively explore how groupthink, chronicity, and strong emotional affect are related to health measures and overall wellbeing. By understanding these relationships, organizations can make informed decisions to improve group dynamics, enhance employee satisfaction, and foster healthier work environments.
In particular, our research illuminated the following key findings
Group Think (Contagious) Dynamics: We found that the propagation of prejudiced beliefs and discriminatory attitudes within groups tends to be contagious. Individuals often conform to the viewpoints of their peers, leading to an amplification of biased perspectives and fostering an environment conducive to hatred.
Chronicity and Enduring Hatred: Chronic exposure to hatred-inducing content and experiences significantly contributes to the perpetuation of hatred. Over time, these negative influences become deeply ingrained within individuals and groups, making it increasingly challenging to disengage from hateful ideologies.
Strong Affect (Extreme-Severe) Amplification: The presence of strong emotional responses, particularly those categorized as Extreme-Severe, further intensifies the impact of hatred. These emotional states can fuel aggressive actions and encourage individuals to adopt extreme positions, resulting in a dangerous escalation of hostilities.
Considering the implications of these findings, we urge the United Nations to take a proactive stance in addressing the interconnectedness of group think (contagious), chronicity, and strong affect (Extreme-Severe) in the context of combating hatred and fostering global harmony. We propose the establishment of a specialized task force or initiative that concentrates on developing targeted interventions and educational programs aimed at:
Disrupting Group Think Dynamics: Promoting critical thinking and media literacy skills to empower individuals to challenge and resist the contagious spread of prejudiced beliefs within group settings.
Breaking the Cycle of Chronic Hatred: Implementing sustained efforts to counteract chronic exposure to hateful content by promoting diverse and inclusive narratives that encourage understanding and empathy.
Mitigating Extreme Emotional Responses: Designing initiatives to address strong affective responses through emotional intelligence training, conflict resolution strategies, and fostering environments that encourage constructive dialogue.
We believe that by addressing these critical interconnections, we can make significant strides toward building a world that values diversity, promotes understanding, and stands against all forms of hatred. We kindly request your support and advocacy in championing these measures within the United Nations framework.
Conclusion
Conceptualizing hatred from a public health perspective in the context of the available epidemiological evidence suggests that hatred is a prominent public health issue that requires attention to the global academic, medical, governmental, and legal institutions. Both as a contagious disease and determinant of health, there is strong impetus to progress from managing hatred to preventing its root causes to promote public health. Understanding the socio- epidemiology and pathophysiology of hatred calls for a multidisciplinary approach, while addressing the triggers and modifiable risk factors of hatred urge for developing holistic, multisectoral, comprehensive, and collaborative approaches to prevent the spread of this phenomenon. There is more to be done to determine risk factors for who is susceptible to (or resistant to) hatred and in relation to the context in which it occurs, and how to measure it.
This study contributes to advance the literature on hatred by suggesting the inter-correlations between constructs that conceptualize hatred as contagious, chronic, and extreme. Based on our theoretical definition of hatred and the results from this study, it is apparent that the best fit model shows significance for hatred as common to the three constructs, contagion, chronicity, and extreme/severe. Hatred is contagious, associated with high levels of group think, which spread rapidly, especially when the object of hatred is also contaminated, i.e., one hates the other.
Acknowledgments
I would like to acknowledge the help and support of Sara Tamjidi in finalizing the preparation of this article for publication.
References
- 1.Halperin E. (2008) Group-based hatred in intractable conflict in Israel. , Journal of Conflict Resolution 52(5), 713-736.
- 3.Cardozo L, Vergara A, Agani F, Gotway A. (2000) Mental health, social functioning, and attitudes of Kosovar Albanians following the war in. 284(5), 569-577.
- 4.Cardozo B, Kaiser R, Gotway C, Agani F. (2003) Mental health, social functioning, and feelings of hatred and revenge of Kosovar Albanians one year after the war in Kosovo. , Journal of Traumatic Stress: Official Publication of The International Society for Traumatic Stress Studies 16(4), 351-360.
- 5.Levin J, Idler E. (2018) Islamophobia and the public health implications of religious hatred. , American journal of public health 108(6), 718.
- 6.Loftin C. (1986) Assaultive violence as a contagious social process. , Bulletin of the New York Academy of Medicine 62(5), 550.
- 7.Abrutyn S, Mueller A. (2014) Are suicidal behaviors contagious in adolescence? Using longitudinal data to examine suicide suggestion. , American Sociological Review 79(2), 211-227.
- 8.Degoey P. (2000) Contagious justice: Exploring the social construction of justice in organizations. Research in organizational behavior 22, 51-102.
- 9.Barsade S. (2002) The ripple effect: Emotional contagion and its influence on group behavior. Administrative science quarterly. 47(4), 644-675.
- 10.Mason C, Griffin A. (2002) Grouptask satisfaction: Applying the construct of job satisfaction to groups. , Small Group Research 33(3), 271-312.
- 11.O’neill J, Harrison M, Cleveland J, Almeida D, Stawski R et al. (2009) Work–family climate, organizational commitment, and turnover: Multilevel contagion effects of leaders. , Journal of Vocational Behavior 74(1), 18-29.
- 12.Felps W, Mitchell T, Hekman D, Lee T, Holtom B et al. (2009) Turnover contagion: How coworkers' job embeddedness and job search behaviors influence quitting. Academy of management journal. 52(3), 545-561.
- 13.Balkhair A. (2020) COVID-19 pandemic: a new chapter in the history of infectious diseases. , Oman medical journal 35(2), 123.
- 14.Abuelaish. (2021) Why hatred should be considered a contagious disease. The conversation. , Published:
- 15.Abuelaish I. (2023) Hatred is a contagious disease and public health issue in ethnopolitical conflicts. In Routledge Handbook of Peacebuilding and Ethnic Conflict 59-70.
- 16.Iacoboni M. (2013) Forum on Global Violence Prevention; Board on Global Health; Institute of Medicine; National Research Council. Contagion of Violence: Workshop Summary. Washington (DC):. National Academies Press (US); 2013 Feb 6. II.5, THE POTENTIAL ROLE OF MIRROR NEURONS IN THE CONTAGION OF VIOLENCE. Available from:https://www.ncbi.nlm.nih.gov/books/NBK207238/ .
- 19.Cacioppo T, Berntson G, Sheridan F, McClintock K. (2000) Multilevel integrative analyses of human behavior: Social neuroscience and the complementing nature of social and biological approaches. , Psychological Bulletin 126(6), 829-843.
- 20.Rueda A, Haisch B. (1998) Inertia as reaction of the vacuum to accelerated motion. , Physics Letters A 240(3), 115-126.
- 21.Savinainen A, Scott P, Viiri J. (2005) Using a bridging representation and social interactions to foster conceptual change: Designing and evaluating an instructional sequence for Newton's third law. , Science Education 89(2), 175-195.
- 22.Russell A, Salem A, Scherer R, Banse R, G Hatfield Wallbott et al. (1994) Emotional Contagion. New York:. , New York: Oxford, Rimbaud. Bulletin de Méthodologie Sociologique 13, 53-90.
- 24.Sapkota P, Brunet A, Kirmayer J. (2020) Characteristics of adolescents affected by mass psychogenic illness outbreaks in schools in nepal: A case-control study. , Frontiers in Psychiatry 11, 493094.
- 25.Glaeser L. (2005) The political economy of hatred. , The Quarterly Journal of Economics 120(1), 45-86.
- 26.Slutkin G. (2013) Forum on Global Violence Prevention; Board on Global Health; Institute of Medicine; National Research Council. Contagion of Violence: Workshop Summary. Washington (DC):. National Academies Press (US); 2013 Feb 6. II.9, VIOLENCE IS A CONTAGIOUS DISEASE. Available from:https://www.ncbi.nlm.nih.gov/books/NBK207245/ .
- 27.Vandenbogaerde E, E Van Hellemont. (2016) Fear and retaliation: Gang violence in Brussels and Caracas. Gang Transitions and Transformations. in an International Context 51-63.
- 28.Bond M, B J. (2017) The contagious spread of violence among US adolescents through social networks. , American journal of public health 107(2), 288-294.
- 29.David-Ferdon C, Simon R. National Center for Injury Prevention and Control, Centers for Disease Control and Prevention (2014) Preventing youth violence: Opportunities for action. , Atlanta, GA:
- 30.Bushman J, Newman K, Calvert L, Downey G, Dredze M et al. (2016) Youth violence: What we know and what we need to know. , American Psychologist 71(1), 17.
- 33.Engel G L. (1980) The clinical application of the biopsychosocial model. , Am J Psychiatry 137, 535-44.
- 34.R H Adler. (2009) Engel's biopsychosocial model is still relevant today. , Journal of psychosomatic research 67(6), 607-611.
- 35.D T Wade, P W Halligan. (2017) The biopsychosocial model of illness: a model whose time has come. Clinical rehabilitation. 31(8), 995-1004.
- 37.Y J Johnson‐Walker, J B Kaneene. (2018) Epidemiology: Science as a tool to inform one health policy. Beyond one health: From recognition to results. 1-30.
- 38.White Halbert. (1980) A Heteroscedasticity-Consistent Covariance Matrix Estimator and a Direct Test for Heteroscedasticity". Econometrica.48(4): 817–838
- 39.Peter J Huber. (1967) The behavior of maximum likelihood estimates under nonstandard conditions. Proceedings of the fifth Berkeley symposium on mathematical statistics and probability 1(1).
- 40.Hu Li‐tze, Peter M Bentler. (1999) Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural equation modeling: a multidisciplinary journal 6(1):. 1-55.
- 41.Engebretson J, Mahoney J, E D Carlson. (2008) Cultural competence in the era of evidence-based practice. , Journal of Professional Nursing 24(3), 172-178.
- 42.J, Reiter-Palmon R. (2008) Responding destructively in leadership situations: The role of personal values and problem construction. , Journal of Business Ethics 82, 251-272.