
Review of Useful Theories for Working with People Who are Living with HIV and AIDS
Abstract
Introduction
Working with people who are HIV positive is a herculean task and relevant theories to assist them medically, psychologically, economically, socially and otherwise are necessary. People who are living positively with HIV and AIDS are usually ridiculed, discriminated against, rejected and isolated. Using theories to work with them will help to cushion the negative impacts of HIV and AIDS, especially stigma which has been identified as a major barrier to health care and quality of life in illness management. The fundamental human rights of people living positively with HIV and AIDS should be protected since majority of such rights are usually trampled upon. The review aimed at discussing the potential benefits of using theories to assist people living positively with HIV and AIDS to cope with their various and varying situations in life.
Materials and Method:
Information for this study was collected by extensive review of recent literature on theories for assisting people living positively with HIV and AIDS. The paper reviews theories that influence long-term behaviour change among people living positively with HIV and AIDS. It assesses the need for using these theories to improve HIV and AIDS intervention in developing countries including Nigeria. In this study, eleven behaviour theories were reviewed.
Result
It was noted that some of the theories promoted adherence as well as helped to explain the benefits of adherence to HIV and AIDS medication. Also a good number of the theories assisted researchers in designing effective intervention strategies.
Conclusion:
Further research is needed to determine the effective theories that will increase adherence to long-term treatment regimens of HIV and AIDS. Such theories can be used to alleviate the potential burnout of Caregivers and people living positively with HIV and AIDS who travel long distances for diagnostic procedures and work long hours without adequate remuneration, support and supervision.
Author Contributions
Academic Editor: Larance Ronsard, National Institute of Immunology, New Delhi-110067.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2016 Enwereji E. E., et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Competing interests
The authors have declared that no competing interests exist.
Citation:
Introduction:
Several theories have been used to address the obvious and emerging problems of people living with HIV and AIDS. Theories assist in the design of behaviour change interventions in HIV and AIDS work 1, 2. Theories promote understanding of the benefits of positive health behaviour, adherence to HIV and AIDS to medical regimen as well as facilitate research in HIV and AIDS intervention and other health issues3, 4, 5. How to ensure that people living positively with HIV and AIDS observe treatment adherence presents challenge to health initiatives 6, 7. Adherence has been defined by 8 as "the extent to which patients follow the instructions they are given for prescribed treatments". Adherence is viewed as a more neutral term than 'compliance', because compliance can be construed as being judgmental 9. Evidence has shown that programmes that promote adherence usually focus on health behaviours 10, 11, 12. This review focused on long-term adherence to HIV and AIDS treatments. Undoubtedly, non-adherence to HIV and AIDS treatment has severe human, economic and social costs. An interrupted treatment may reduce treatment efficacy and cause drug resistance 13, 14, 15, which can result to increased morbidity, mortality and further infections. Without intervention, adherence rates to long-term medication in high income countries are approximately 50% 16, while adherence rates in low and middle income countries are even lower 17.
Chronic and infectious diseases like TB and HIV that affect mainly the disadvantaged populations and involve complex treatment regimens with potential severe side effects present challenges to adherence 18. However, both are public health priorities and non-adherence to their medications may cause drug resistance and/or failure 19. Their characteristics of complex treatment is what differentiates them from other chronic diseases such as asthma and hypertension where, for example, drug resistance is not a key issue19, 20. Treatment adherence is affected by beliefs about the origins, transmission and treatment of TB and HIV, which often results to the stigmatisation of those affected 21, 22. The interactions of these factors make adherence for these diseases not only a priority but a complex health issue.
Various theories for interventions have been designed to improve treatment adherence, but only few of the theories described in specific terms the processes involved in using the theories to achieve behaviour change 22, 23 making it difficult to choose the most appropriate theory to design interventions for HIV infection24. This constitutes a problem particularly in developing countries where adherence to long-term medications for chronic and infectious diseases is not guaranteed 24, 25. Therefore, there is need to use existing theories like the transtheoretical, biomedical, behavioural, communication, and cognitive models to enhance long-term medication adherence for people living positively with HIV and AIDS25, 26. However, research has shown that the commonly used theories or models are those of cognitive and transtheoretical models 27, 28, 29, 30, 31, 32. In this review, short descriptions of theories, their characteristics, relevance and applicability to adherence to HIV long-term medications were examined.
This paper is intended to provide useful information for researchers interested in using theories to address the interpersonal factors that affect treatment adherence and reduce HIV infection among HIV positive individuals. However, there is evidence that well designed and targeted theory-based behaviour change interventions can be effective in reducing the spread of HIV. It will also help to improve the self-esteem of those living positively with HIV and AIDS.
Methods
Extensive review of relevant literature was done. Experts were also consulted for comments and references. Articles that described interventions related to HIV and AIDS adherence to medications was identified and efforts were made to include all available theories. Some of the main advantages and disadvantages of the theories were also highlighted. Eleven theories were reviewed. In this paper the term theory was used to include models.
Results
The details of the findings in the review will be presented according to the perspective of the theory. Diagrammatic representation of some of the theories will also be presented.
The Biomedical Perspective
The biomedical perspective integrates the biomedical theory. Here, the patients are expected to be submissive to the doctors’ instructions 28. Disease is implicated with biomedical causes, like bacteria, viruses and others and treatment is focused on the patient's body 29. According to the biomedical theory, illnesses should attract mechanical solutions like prescribed pills or drugs 28. Patient’s non-adherence to medications is attributed to the patient’s characteristics such as age, sex, religion and others and not to medication because technological innovations are meant to promote adherence 29. However, activities like monitoring and evaluation are also rooted in the biomedical perspective 30. Despite the health workers’ purported implicit use of the biomedical perspective, research has shown that this perspective is not explicitly used in most interventions30.
The primary limitation of this theory is that it overlooks factors like patients' perception of their illnesses, psycho-social influences, socio-economic environment but rather views patients’ characteristics as the main factors that influence health behaviours 31, 32. The disadvantage of using demographic variables alone as the main variables that affect adherence is that some groups may be excluded 29. The advantage of this theory is in its flexibility. The biomedical theory has now been included in the larger "biopsycho-socio-environmental" theory, which has wider socio-environmental application for all patients 30. Also the assumption that patients are passive to the doctors’ instruction makes using biomedical theory alone during intervention unlikely to contribute significantly to HIV medication adherence. This is because patients are expected to be active in making decisions about their health and not merely to receive and follow instructions passively.
The Oral Polio Vaccine (OPV) Theory
This theory argues that HIV was transferred iatrogenically or by medical interventions to humans and that polio vaccines played significant role in the transfer of the HIV virus. Edward Hooper hypothesized that in the late 1950s oral polio vaccine called Chat which was cultivated in living tissues of chims was responsible for HIV infection among Africans. Chat was grown in kidney cells taken from local chimps infected with Simian Immunodeficiency Virus (SIV) and as a result a large number of people subsequently became infected with HIV- 1. HIV-1 is termed to be closely related to SIV.
The limitation of this theory is the myth it circulated which negatively affected acceptance of vaccination for polio virus. Overcoming this myth influenced the adoption of oral method as the most appropriate route for polio vaccine administration. Using oral administration for the vaccination of polio is insufficient to cause infections like SIV and HIV which is through the bloodstream. This means that for SIV and HIV to infect humans, they need to enter directly into the bloodstream to cause the infection22. Also the lining of the mouth and throat generally act as good barriers to the virus 21, 25. The advantage of this theory is that it helped to create awareness that it is only the macaque monkey kidney cells, which cannot be infected with SIV or HIV, that were used to make Chat22. This theory helped to explain that HIV existed in humans before the OPV vaccine trials were carried out, and therefore, could not have been a source of HIV infection.
The Contaminated Needle Theory
This theory posits thathealthcareprofessionals, especially in Africa were using one single syringe to inject multiple patients without any sterilization in between the services. As a result, that there was rapid transfer of blood transmitted infections including HIV in health care services. The limitation of this theory is that it propagated the notion that the inability of health workers to sterilize syringes is responsible for the wide spread of SIV and HIV in the society. In other words, that this practice was responsible for the transfer of HIV infection from one individual to another as well as the rise in the mutation of SIV to HIV18. The advantage of the theory is that it created awareness on the need for health workers to sterilize syringes before use. Also, the theory motivated the health workers to adopt single use for syringes.
AIDS Risk Reduction Model
The AIDS Risk Reduction Model believes that change is a process every individual must experience. Though change occurs, but different factors will affect its magnitude, time, direction and others . This model argues that the more an intervention helps clients to progress on the stage continuum, the more likely they are to exhibit change.
This model has several advantages. For instance, the theory integrates elements from other behavior theories/models like health belief model, self-efficacy theory, and psychological theory .The model is very relevant when proffering intervention to sexually active or injecting drug users who are at risk of several infections including sexually transmitted infections like HIV. This model was developed specifically from the context of HIV perception. The model emphasizes that individuals must pass through three stages of the model, labeling stage, commitment stage and enactment stage before achieving risk reduction.
Labeling Stage
Using this model, it is believed that individuals must have knowledge that some of their actions can be a risk factor for HIV infection. Here individuals are expected to know the three elements that are of immense benefits in the theory. These are:
I Knowledge about how HIV is transmitted and prevented.
Ii Perceiving that one can be susceptible to HIV infection.
Iii Believing that HIV is avoidable
Commitment Stage
This is the decision-making stage which could result in one of the following outcomes.
i.Making a firm commitment to deal with the problem positively.
ii.Remaining resolute in avoiding risky behaviours.
iii.Taking actions to ensure that the problem is favourably resolved.
iv.Resigning from the problem by weighing the cost and benefits of giving up pleasure (high risk) and that of less pleasure (low risk).
v.Knowing the major factors which include
Responding to efficacy or effectiveness of change,
perceiving enjoyment as actions to be added or eliminated,
considering the need for self-efficacy, and
need to have relevant information and social norms
Enactment Stage
This stage requires the following three relevant actions to achieve a good result
vi.Seeking useful information,
vii.Obtaining timely remedies, and
viii.Enacting prompt solutions.
The theory argues that if the actions in this stage are religiously followed, that risk reduction will be achieved. The advantage of this theory is that it exposes individuals to the full knowledge of how HIV is transmitted as well as how it can be prevented. The disadvantage of the theory is that those without full knowledge of the transmission and prevention of HIV infection encourage discrimination and rejection of those who are HIV positive.
Behavioural (learning) Perspective
This perspective includes behavioural learning theory (BLT). BLT focuses on the environment by teaching skills on how to manage adherence 17. This theory uses principles of antecedents and consequences to influence behavior change. Here antecedents are either internal (thoughts) or external (environmental cues) while consequences are punishments or rewards for a behaviour. The likelihood of a patient following a particular behaviour depends on the variables in the internal and external environments 17.
The strategies used in this perspective to improve adherence are usually through direct contact reminders to patients on the benefits of their actions 16. Some authors who have used these strategies during intervention have reported effective adherence to long-term medications 24. A recent report on adherence to highly active antiretroviral (ARV) therapy concluded that interventions using cues and external rewards were efficacious 35. However, a randomized controlled trial on ARVs reported a negative effect when electronic reminder systems were used for patients 17.
The main limitation of this theory is that it does not consider the influences of past behaviour, habits,or non-acceptance of behaviours that are not linked to immediate rewards 15. Also another disadvantage of the theory is that it regards behaviour change as more of external influences than internal influences. Researchers argue that for effective use of the theory, that individuals' perceptions of appropriate rewards constitute must be carefully considered22. The advantage of this behavioural theory is in its flexibility during interventions. For a more effective results during interventions, health workers use behavioural theory in combination with other approaches. Below is a diagram to illustrate behavior theory.
Conspiracy Theory
Some believe that HIV is a ‘conspiracy’ or that it is ‘man-made’. Centers for Disease Control and Prevention first reported HIV and AIDS epidemic in 1981,and since then, some reports have it that the virus was created by the CIA to wipe out homosexuals and African Americans. Some even said that the virus was created to expose couples that indulge in extra-marital sex14. Even today, many people uphold the conspiracy theory claiming that the virus originated in Africa and that the U.S. government purposely manufactured the virus in the military laboratories just to punish developing countries especially Africans. Others insist that the U. S. government deliberately injected gay men with the virus during 1978 hepatitis-B experiments in New York, San Francisco and Los Angeles as well as during smallpox inoculation programme. Others from the scientific community believe that the virus was transmitted from monkeys to humans during the 1930s and that a cure for AIDS is being withheld from the poor13.
The limitation of this theory is that individuals especially the homosexuals do not fear engaging in practices that put them at risk of infection because of the view that HIV is a biological warfare programme, designed to wipe out blacks and homosexual people 21. However, there was no effort to disprove this belief because of lack of effective genetic engineering techniques at the time of the emergence of HIV and AIDS. The main advantage of this theory is that it helped to strengthen networks.
Figure 1.Behavioural learning theory (Adapted from Munro et al. BMC Public Health 2007)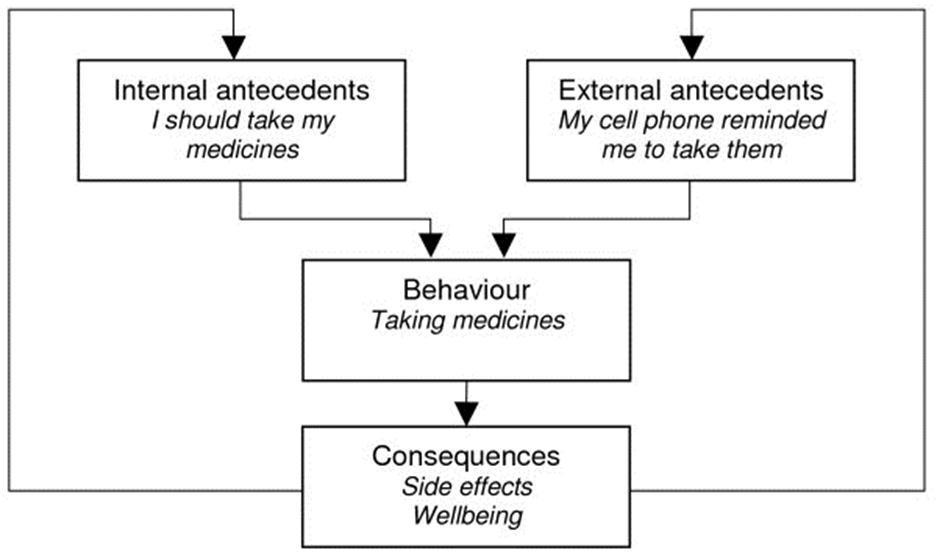
Empowerment Theory
Empowerment theory is a theory that encourages people to change from negative behavior to positive behavior. The theory enables individuals to come together to share experiences, understand social influences, and develop solutions to their problems. In empowerment theory, there are three core elements that make up the theory, populations for change, participatory education, and focus group strategies that are very important.
Populations for change – this is used to discuss and find solutions to problems at individual or group levels.
Participatory education – this helps to develop skills for listening, for engaging in effective participatory dialogue and positive actions.
Focus group strategies –this is for gathering information and finding solutions with the assistance of community members.
The theory believes that the three elements must work in harmony before it can guarantee effective learning and improvement to achieve the desired goals. The limitation of this theory is that the elements that make up the theory do not work in isolation. They must be combined before a meaningful achievement is realized. The advantage of the theory is that each element in the theory is a strength to each other.
The Hunter Theory
The theory is of the view that HIV infected humans through the hunter who killed and ate the meat of chimps. The theory argues that the virus Simian Immunodeficiency Virus (SIV) came from the chimps and gained quick entry into the human system when the blood of the chimp mixed with the blood of the hunter through cuts or wounds on the hunter’s body. The theory posits that as a result of this entry, SIV adapted itself with the blood of the new human host and became HIV. The theory further argues that each time SIV from a chimpanzee enters the human body, that it produces a slightly different strain 9. Ideally, the hunter’s body could have resisted SIV infection, but for the fact that SIV readily adapts itself with the new human host to become HIV-1. The theory emphasizes that there are several strains of HIV, and that each with a different genetic make-up especially that of HIV-1 group M. This means that every time SIV passes from chimpanzee to man, a different strain will be produced 7, 21. Unfortunately, despite the traits of zoonatic diseases, individuals especially in developing countries still favour bush meat as a delicacy. Some researchers have advised that eating of bush meat especially chimpanzee so as to prevent infections of simian viruses to humans 13.
The main limitation of this theory is that the harsh economic conditions of individuals in developing countries where food is not easily available and many people rely on bush meat as sources of income and protein intake makes it difficult for them to adhere to the advice of avoiding bush meat. Eating of bush meat especially chimpanzee exposes people to SIV infection.
Communication Perspective Theory
Communication is the key to patient-health worker’s relationship 14. The theory suggests that effective communication with clients will enhance adherence 8, 10. The theory emphasizes that adherence can only be achieved if clear and comprehensive patient education is provided by a health care worker with good communication skills25. The theory emphasizes the need for patient education to include the timing of treatment, instruction to avoid possible recurrence, and comprehension of the intervention provided. An effective intervention should aims at improving client-provider interaction 18. The theory believes that communication can be used as intervention strategy to increase adherence 21.
The limitation of this theory is that it ignores attitudinal, motivational and interpersonal factors that could interfere with the messages clients receive and translate to produce behaviour change 12. The advantage of this theory is that it encourages good patient- health worker interaction.
Diffusion of Innovation Model
The Diffusion of Innovation Model looks at how effective new ideas are communicated to clients, and how such ideas are accepted by them. There are three major components of this theory, communication Channels, opinion leaders, and time and process.
Communication Channels, these are needed to enable health workers dispense innovative and new messages effectively.
Opinion Leaders, these are well respected individuals in the society who can assist health workers to dispense messages efficiently and effectively.
Time and Process, they are needed in other to meet the needs of the clients because clients receive and accept messages at different time intervals. The ability to accept messages depends on the process used for the communication. The advantage of this theory is that communication gaps which can negatively affect behaviour change are avoided.
Cognitive Perspective
Cognitive perspective includes theories like social-cognitive theory (SCT), health belief model (HBM) and other theories that focus on cognitive variables as part of behaviour change. The theories in cognitive perspective share the assumption that attitudes and beliefs are the expectations of future events and outcomes and also are the major determinants of health related behavior change. The theories argue that in the face of various alternative variables, that individuals will choose the actions that will lead them to positive outcomes 24.
These theories have several limitations. The theories do not include factors like power relationships and social reputations that may influence adherence to behaviour change 25. Also the theories ignore the fact that risk behaviours can affect more than one person, and did not pay attention to additional risks that may affect the interventions provided 24.
The protection-motivation theory
According to this theory, behaviour change may be achieved by allaying an individual's fears. The theory has three important types of fears, the magnitude of harm of the depicted event; the probability of the event’s occurrence; and the efficacy of the protective response that must be allayed before behavior change can take place. The three types of fears when combined will show how effective the protection motivation theory is during intervention 19, especially if the intervention is on the desire to protect against danger 23.
The theory has the advantage of being the only theory in the cognitive perspective that uses costs and benefits of recommended behaviour to predict change 29. The theory assumes that motivation to protect self from danger is a positive function of beliefs that sees the threat as severe and individually vulnerable. The theory views beliefs as health-impairing behaviour that is capable of rewarding but costly to give up and can also assume a negative effect 22. Another advantage of this theory is that it moderates behaviour 30 and as such, the theory is appropriate for adherence to long-term medications but the theory does not assume that behaviour is always rational 31. The limitation of this theory centers on its inability to identify variables that conform to social norms as well as the environmental and cognitive variables that may influence attitudes 25. Therefore, researchers have advised that those using this theory for intervention, should take cognizance of the influences of social, psychological and environmental factors on motivation 31, 32, 33.
Health Belief Model (HBM)
This model views change in health behaviour as a product of the objective appraisal of the barriers and benefits of action 12, 13. According to this model, the perceived seriousness of, and susceptibility to a disease will influence the individual's perceived threat of the disease. Also, the perceived benefits and the perceived barriers will influence the perceptions of the effectiveness of a health behaviour. At the same time, demographic and socio-psychological variables will influence perceived susceptibility and perceived seriousness, as well as the perceived benefits and perceived barriers to action 4, 10. The theory argues that perceived threats is influenced by cues to action, which may be either internal cues like symptoms the individuals perceive or external cues like health communication.
The theory is of the view that increase in perceived threats, and perceived benefits will result to less barriers to action and also encourage one to engage in recommended behaviours 12.
In using this model, all the components of the theory are termed as independent predictors of change in health behaviour 11, 28. However, perceived threats especially perceived severity have poor correlation with health actions and can negatively affect taking protective actions. Perceived severity is not seen as important as perceived susceptibility and this is why the theory stresses on self-efficacy so as to enable individuals feel competent to influence long-term change 11.
The theory has some limitations when used during intervention. The theory does not shows the relationships between the variables or provide clear rules on how to combine the variables for a better result during intervention 28. The theory assumes that the variables are not affected by each other but that they only have a stabilizing effect 32. HBM also assumes that variables affect health behaviour directly and will remain unchanged by behavioural intentions 22. Another limitation of the theory is that the theory isolated important social influences on determinants of health behavior 22, 32. For instance, smoking, which is more of habit than decision, has not been properly explained in this case. The theory predicts adherence in some situations, but did not clearly explain risk reduction behaviours which are linked to socially determined and unconscious motivations 12.
Therefore studies are needed to assess the validity of this theory in adherence to long-term medications for HIV and AIDS 4, 11. This is necessary because when applying this theory to long-term medication adherence, it is essential to consider the influences of the socio-psychological factor like cultural beliefs otherwise, the effectiveness of the theory during interventions may not be clear.
However, the Health Belief Model holds the view that positive change in health related behaviours will occur only when perceived susceptibility, perceived severity, perceived benefits, and perceived barriers are attained.
Perceived susceptibility, which is knowing that one can be personally vulnerable to that condition.
Perceived severity, that is, the belief that harm can be done by the condition.
Perceived benefits of performing a behaviour , that is the gain one can get from the change.
Perceived barriers of performing the behaviour, that is, factors that prevent one from changing.
Below is the figure 4 representing health belief model and other theories.
Figure 2.Revised protection motivation theory (Munro et al. BMC Public Health 2007 7:104).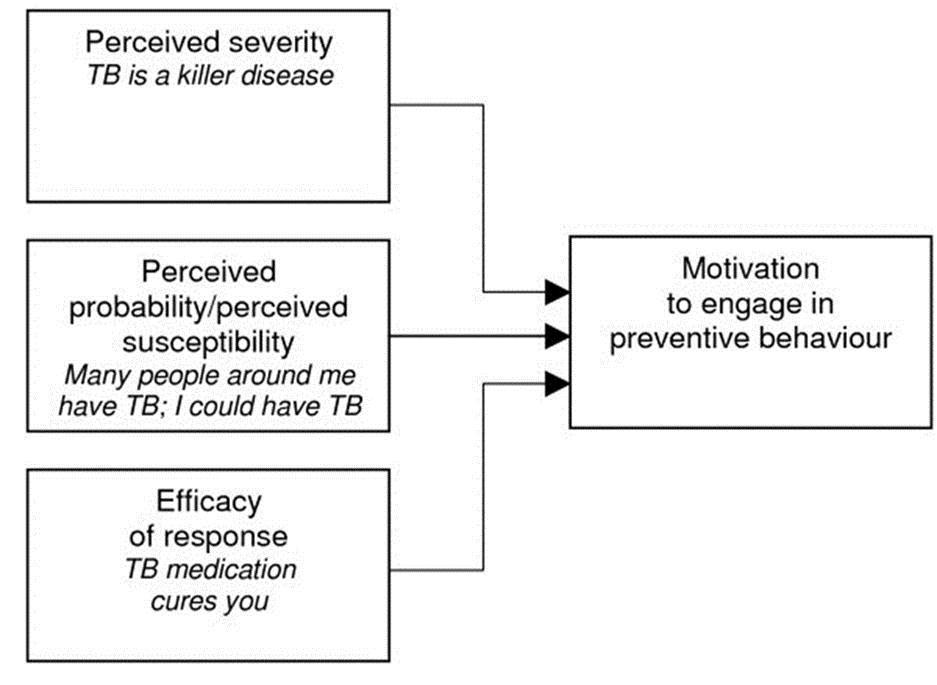
Figure 3.Revised protection motivation theory (Munro et al. BMC Public Health 2007 7:104).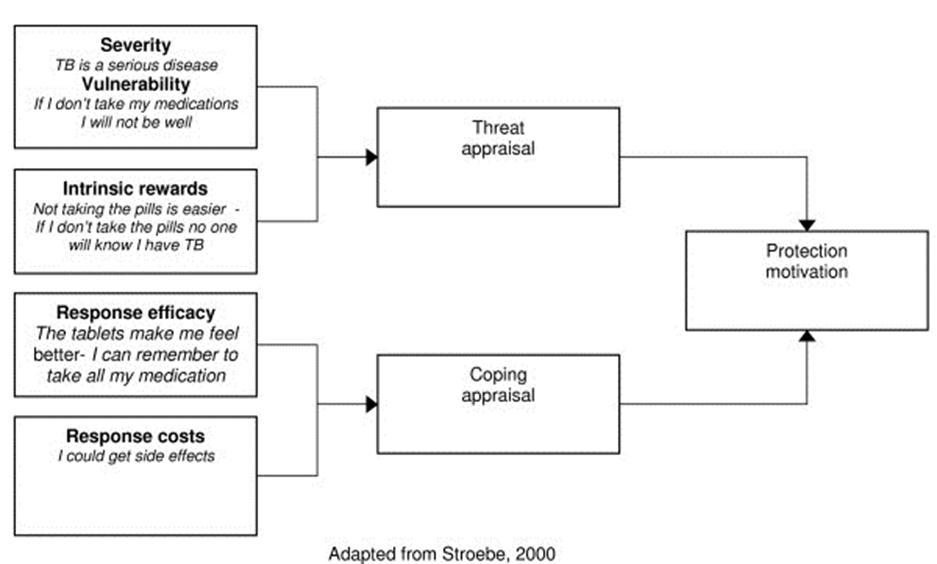
Social Cognitive Theory
The Social Cognitive Theory believes that behaviour changes are dynamic and can be influenced by personal and environmental factors. The theory argues that people will learn new behaviours by experience, and by modeling others after observation. That ability to achieve the required change will depend upon the following:
Outcome expectations, that is , the extent to which the person values the expected outcome of a specific behaviour. The question is: Will the behaviour lead to a positive or negative outcome?
Self efficacy, that is the person’s belief about the ability and confidence to carry out the expected behaviours
This theory which evolved from social learning theory has the advantage of being the most comprehensive theories of behaviour change that has so far been developed 1. The theory posits that there are complex but causal factors in human motivation, action and well-being. The theory provides predictors for adherence as well as the guidelines for behaviour change 26. The theory proposes that the principle of behaviour change is a reciprocal that has continuous and dynamic interaction between the individual, the environment and behaviour 1.
The theory views knowledge of health risks, benefits of positive actions, and self-influences as the prerequisite for change to occur 21. Beliefs about self efficacy help to influence, and play central roles in the behavior change. Change in health behaviour is affected by positive and negative effects of material losses and benefits. Behaviour change outcomes are said to attract social approval or disapproval for an action. How individuals assess the positive and negative self-evaluations of their health behaviour and health status can influence their outcome behaviour. Other important determinants of behaviour change include perceived facilitations and barriers because behaviour change is as a result of the reduction or elimination of barriers 17. In summary, this theory proposes that behaviours are taken when people are confident that they have control over the outcome of their behaviours 28.
Some authors believe that self efficacy can explain between 4% to 26% of variances in behaviour 23. The limitation of this theory is that it has wide-range focus, and as such, difficult to operationalize during interventions. As a result, it is only used in parts 22, 25, thereby raising some questions as to its applicability to intervention development.
Figure 4.Health Belief Model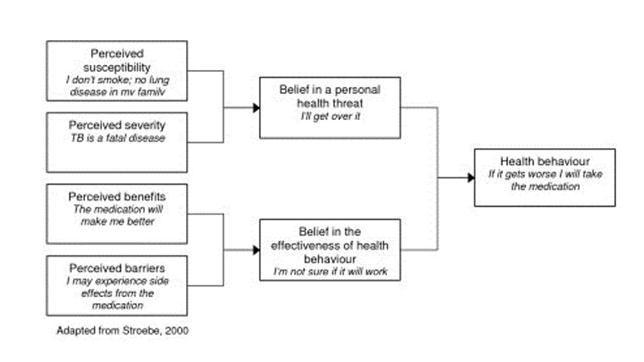
Theory of Planned Behavior (TPB) and the Theory of Reasoned Action (TRA):
The first work in this perspective was that of the TRA 13, 24. The TRA argues that most socially relevant behaviours are under volitional control, and that a person's intention to perform a particular behaviour is the immediate determinant and the single best predictor of that behaviour 25 This theory stipulates that behaviour is influenced by ones attitudes, beliefs and evaluations of the outcome of the behavior. That is whether the outcome of the actions will be positive or negative, subjective or objective. The theory believes that actions are also influenced by the perceived expectations of important others in the family or in the work place , and that motivation is derived by complying with others' wishes and behavioural intentions. Some authors argue that variables apart from those described above, can only influence behavior positively if such variables influence attitudes or subjective norms 14. This suggests that support for using this theory during interventions is restricted.
Further, TRA does not believe that behaviours are not always under volitional control as well as past behaviours having impact on current behaviours21. As a result of this, the proponents of this TRA included behavioural control in the theory and called it theory of planned behavior (TPB). Here, behavioural control represents the perceived ease or the difficulty in performing the behaviour and is a function that will controls beliefs 13.
Conceptually TPB is very similar to self-efficacy 22 and includes knowledge of relevant skills, experience, emotions, past track records and external circumstances 14. Behavioural control is assumed to have a direct influence on intentions 15.
The limitations of these theories are largely dependent on rational processes. The theories do not show the impacts of emotions or religious beliefs on a stigmatised disease like HIV and AIDS.
Figure 5.social cognitive theory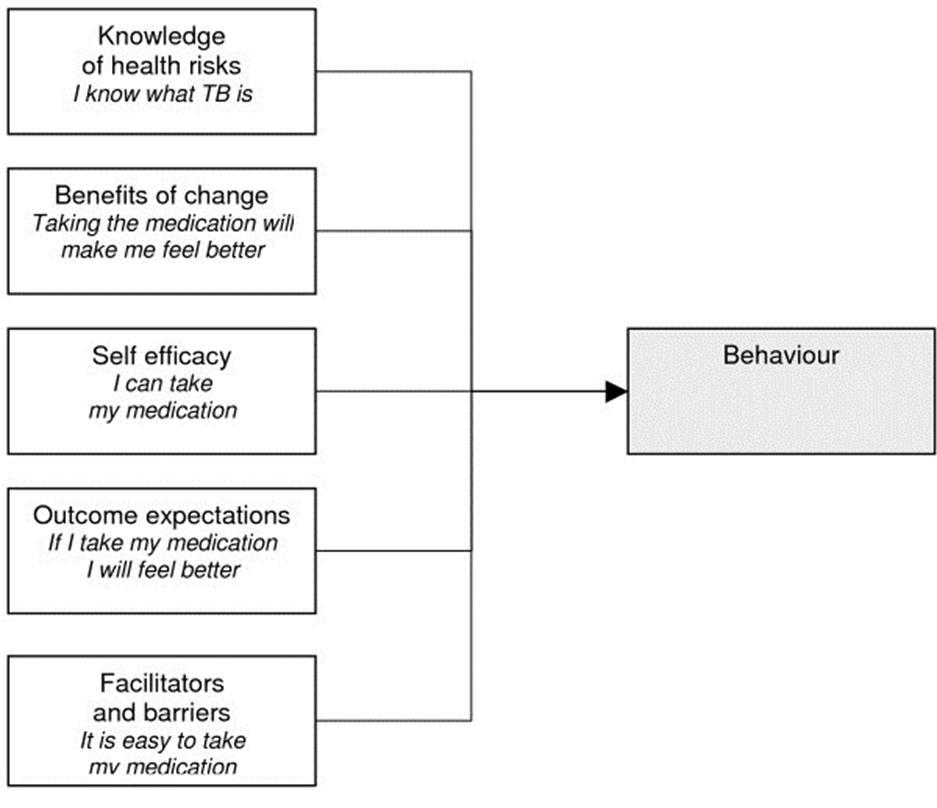
Figure 6.Theory of reasoned action (TRA)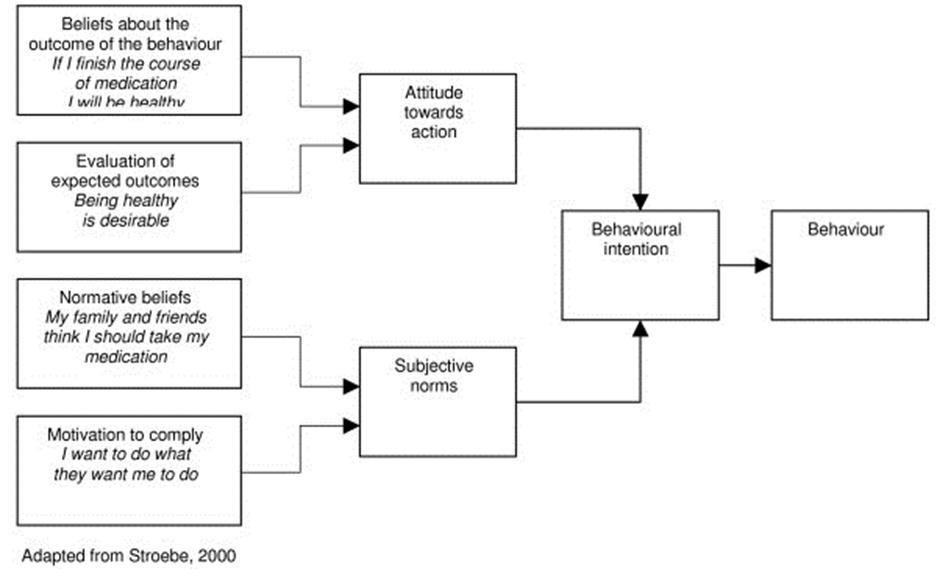
Figure 7.Theory of planned behavior (TPB)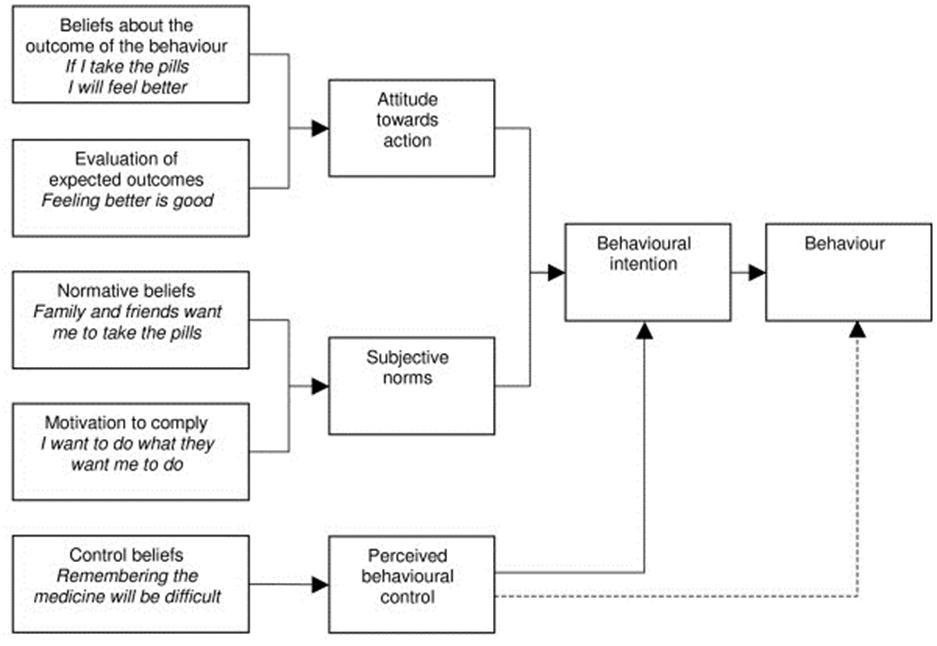
Information-Motivation-Behavioural Skills (IMB) Theory:
This theory was developed to promote contraceptive use and prevent HIV transmission. The theory has the advantage of being simple, generalizable and conceptually based to promote HIV prevention 19. The theory is specifically adapted to design interventions to promote adherence to ART 25.
The theory projects three factors, information, motivation and behaviour skills as very important in the improvement of behavior change. Information as recorded in this theory refers to the basic knowledge about a medical condition, and is a necessary requirement for behaviour change. An effective intervention will begin with the baseline information, and avoid information gaps 25. For motivation, the theory views personal attitudes towards adherence, perceived social supports, the patients' subjective norms, the patients’ perception of how others with similar condition behave, sense of self-efficacy and the belief that the recommended behaviour can be achieved as sources of motivation 25. In behavioural skills, the theory regards factors such as ensuring that the patients have the requisite skills, tools and strategies to perform the needed behaviour as well as possess sense of self-efficacy as important behavior skills to attain good behavior25.
Using this theory, the factors are moderated by a range of contextual conditions such as living conditions, access to health services and access to information. These contextual conditions are seen as capable of motivating activate behavioural skills that will result in risk reduction, behavioural change and maintenance of positive behaviours 5, 25. The advantage of IMB is that it is effective in promoting positive behaviour change and also has some predictive value for ART adherence 7. Also, it is simple to use and has the potentials to increase ART adherence. Some authors believe that the theory is a promising model that is capable of promoting adherence to long-term medications 5. However, there is need to assessed the effects of this model on clients.
Self-Regulation Perspectives
Self-regulatory theory is an important theory developed to conceptualize focus on the patients’ adherence processes 28. The theory proposes the need to examine how individuals are exposed to health hazards and also how they understand the way in which health threats can be adapted. According to this theory, individuals with negative emotional responses encounter cognitive problems of health threats and have difficulty in combining new information with past experiences unlike those with positive emotions 15. The theory posits that the type of emotional responses individuals possess will determine the strategies to cope with health threats that will influence positive outcomes 26. The theory assumes that people avoid illness threats because they are active and self-regulating problem solvers 17. The theory argues that people attain a state of internal equilibrium by testing the efficacy of coping strategies.
The process of creating health threats or risk factors and choosing appropriate coping strategies is dynamic and informed by an individual's demographic, social and cultural variables 15. However, studies have shown complex interplay between environmental factors and symptoms and beliefs about disease aetiology 6. The limitation of this theory is that it is not very useful in designing interventions 7. There is need for more research to identify how to utilize the processes in the theory to promote adherence to long-term medications.
Stage Perspectives:
The Transtheoretical Model (TTM)
This theory is the most prominent among all the theories in the stage perspectives. The theory hypothesizes why people with different discrete stages and processes move through the stages with relapses and only achieve success when earlier stages are revisited 8, 9. The theory offers different processes at different stages and suggests that the process of change is determined by assessing the covert and overt activities that help individuals to attain healthier behaviours.
The disadvantage of this theory is that it lacks clear definition of the stages of change and the extent of coverage. The theory also has little information on how people change and why some people succeed while others fail. According to 11, the theory defy the three basic assumptions of stage theories, that is, qualitative transformations across discrete stages, invariant sequence of change, and non-reversibility. Studies by 11 suggests that the functions of the human body is too multifaceted that it cannot fit into separate, and discrete stages. It further stated that stage thinking could limit the scope of change-promoting interventions.
Figure 8.Information motivation behavioural skills model.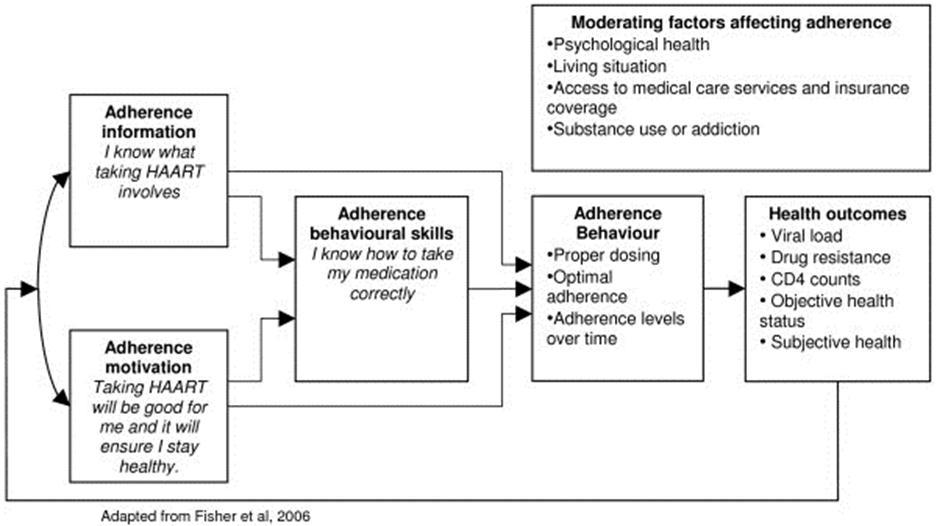
Therefore, the stage definitions in the theory are logically flawed, and time periods assigned to each stage are arbitrary16. As a result, more attention on measurements, testing of issues and definition of variables with their resultant causal relationships is needed 18. This shows that the coverage and types of processes included in this theory are inadequate 6.
The advantage of the theory is that interventions are tailored toward individual needs unlike other theories. However, the theory is more appropriate where rapid behaviour change is not necessary.
Figure 9.Self regulation theory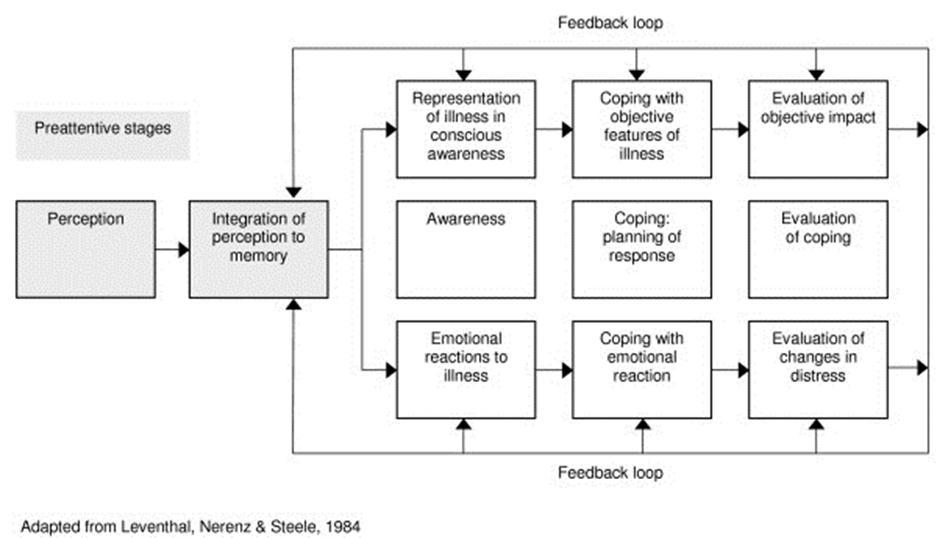
The Colonialism Theory:
Colonial rule in Africa was harsh and many Africans were kept in labour camps where sanitation was poor, food was scarce and physical demands were excessive. According to this theory, the harsh conditions under which the labourers worked exposed them to poor health. As a result, SIV invaded the weak immune system and become HIV. Most researchers were of the view that since food was scarce among the labourers, that it was likely that chimpanzee which transmits SIV, must have formed part of the food served the labourers21. Also, to protect the workers from infectious diseases like smallpox, hepatitis and others, the workers were inoculated with unsterile needles which further exposed them to blood transmitted infections 12, 33. The theory argues that because the labours were camped around the period HIV was found among humans 34, 35, 36 and moreover, as a form of relaxation, the labourers were allowed free access to prostitutes5, helped to expose the workers to HIV infection.
Discussion
This review explains a number of health behaviour theories that can contribute to adherence to long-term medications of HIV and AIDS. Using theories to develop interventions to promote adherence for long-term medications among people living with HIV and AIDS will offer several advantages, but there are also some limitations. There is little or no evidence on how to compare these theories for more effective result 16. Combining theories to achieve a better result in predicting behaviours is worthy but this requires tact because of the various methodological problems in the original theories. Several theories have been propounded in HIV and AIDS interventions and theorists have continued to examine and re-examine the effectiveness of the theories in several areas of behaviour using existing explanatory theories.
Researchers, health workers and health planners are overwhelmed by the multitude of available theories in health work. Some of these theories are fragmented, contradictory and some discredited. The question is, can these theories be used in other health interventions apart from in the context which they were developed? Some authors argue that most theories in HIV and AIDS did not address sufficiently the socio-cultural and psychological aspects of HIV prevention like stigma, rejection discrimination and others. Issues such as these that are associated with HIV and AIDS especially in developing countries could affect the acceptability and uptake of interventions. Another question is whether theories propounded in developed countries where HIV burden is low, are applicable to individuals in developing countries where the disease burdens from HIV and AIDS are high.
According to several authors, health behaviour change theories include varieties of health behaviours, and each is qualitatively different from the other in improving adherence to specific health behaviours7, 3. For example, adherence to long-term medications in HIV and AIDS will be different to a behaviour change in multiple sex partners 36. However, achieving increased adherence to HIV and AIDS medication may be seen as an important public health issue because of its infectiousness, and the recent emergence of drug resistant strains 8. It is therefore difficult to compare the effectiveness of the theories in health care services using individual categories.
Using theories to design interventions remains a challenge to researchers and health planners because of the debate on the effectiveness and usefulness of the theories. As a result of this variation, there is no clear evidence in support of any of the theories as the most effective in the field of adherence behaviours but rather, it may be safer to combine the theories for a better effective service. While these debates continue, more research should be done to shed light on the efficacy of each theory. The questions are, will an effective intervention be a proof of the efficacy of the theory used? How can the efficacy of a theory be reliably tested? Some research work has already been undertaken in an area like systematic review of antiretroviral treatment adherence interventions, However, studies by 15, 18 argue that using theories to construct an intervention may not predict the efficacy of the intervention.
Conclusions
The field of health behaviour theory remains dynamic, and it is important to continue developing existing theories and approaches as new evidence emerges. It should be noted that interventions capable of changing adherence behaviour for people living positively with HIV and AIDS, must be located within the relevant social, psychological, economic and physical environments because there is no simple solution to the problem of adherence, or behaviour change even though health behaviour theories may shed light on the processes underlying behaviour change.
However, since theories have practical behaviour change potentials, and since the problem of medication adherence remains significant for both clinical medicine and public health, further exploratory and explanatory research is needed. Given the importance of long-term medication adherence to global public health, particularly in relation to the HIV epidemics, such research should receive much higher priority. This review provides useful information for those who are interested in working with people living positively with HIV and AIDS.
Recommendations:
However, some recommendations have been suggested to address the difficulties encountered by the multiplicity of theories on health behaviour change. The followings are therefore recommended to improve the efficacy of some theories:
1.Variables that are common to all the theories should be highlighted so as to avoid duplication of variables.
2.Psychological theories that will help to build and stabilize the emotional wellbeing of HIV positive individuals should be made more accessible and easier to use during interventions.
3.Guidance should be provided on the important variables in the psychological theories that are capable of addressing discrimination and rejection of people who are HIV positive.
4. Theories should be integrated to enable researchers and theorists avoid proliferation of redundant variables This is because some theories share overlapping variables that are described with different names.
References
- 1.Dunbar J M, Marshall G D, Hovell M F. (1979) Behavioural strategies for improving compliance. In Compliance in health care. Edited by Haynes RB,Taylor DW,Sackett DL.Baltimore:JohnsHopkinsUniversityPress. 174-190.
- 2.Simoni J M, Pearson C R, Pantalone D W, Marks G, Crepaz N. (2006) Efficacy of interventions in improving highly active antiretroviral therapy adherence and HIV-1 RNA viral load: a meta-analytic review of randomized controlled trials. , J Acquir Immune Defic Syndr43(Suppl 1, 23-35.
- 3.Mannheimer S B, Morse E, Matts J P, Andrews L, Child C et al. (2006) Sustained benefit from a long-term antiretroviral adherence intervention: results of a large randomized clinical trial. , J Acquir Immune Defic Syndr.43(Suppl 1, 41-47.
- 4.Rosenstock I M, Strecher V J, Becker M H. (1988) Social learning theory and the health belief model. , Health Educ Q 15, 175-183.
- 5.Posse M, Baltussen R. (2009) Barriers to access to antiretroviral treatment in Mozambique, as perceived by patients and health workers in urban and rura settings. , AIDS Patient Care STDS 23, 867-875.
- 6.Tuldra A, Fumaz C R, Ferrer M J, Bayes R, Arno A et al. (2000) Prospective randomised two-arm controlled study to determine the efficacy of a specific intervention to improve long-term adherence to highly active antiretroviral therapy. , J Acquir Immune Defic Syndr 25, 221-228.
- 7.Armitage C J, Conner M. (2002) Reducing fat intake: Interventions based on the theory of planned behaviour.In Changing health behaviour.Edited by Rutter D, Quine L.Buckingham:OpenUniversityPress;. 87-104.
- 8.NCM Theunissen, DTD deRidder, Bensing J M, GEHM Rutten. (2003) Manipulation of patient-provider interaction: discussing illness representations or action plans concerning adherence. , Patient Educ Couns 51, 247-258.
- 9.Griffin S J, Kinmonth A, MWM Veltman, Gillard S, Grant J et al. (2004) Effect on Health-Related Outcomes of Interventions to Alter the Interaction Between Patients and Practitioners: A Systematic Review of Trials. , Ann Fam Med 2, 595-608.
- 10.Becker M H, Maiman L A, Kirscht J P, Haefner D P, Drachman R H et al. (1979) Patient perceptions and compliance: Recent studies of the Health Belief Model. In Compliance in Health Care.Edited byHaynes RB,Taylor DW,Sackett DL.Baltimore:JohnsHopkinsUniversityPress; 78-109.
- 12.Gebhardt W A, Maes S. (2001) Integrating social-psychological frameworks for health behaviour research. , Am J Health Beh 25, 528-536.
- 13.Mills E, Cooper C, Anema A, Guyatt G.(July2008) "Male circumcision for the prevention of heterosexually acquired HIV infection: a meta-analysis of randomized trials involving 11,050 men". , HIV Med. (Meta-analysis) 9(6), 332-5.
- 14.Fishbein M, Ajzen I. (1975) Belief, attitude intention and behaviour: An introduction to theory and research.Menlo Park:Addison-Wesley.
- 15.Eccles M, Grimshaw J, Walker A, Johnston M, Pitts N. (2005) Changing the behavior of healthcare professionals: The use of theory in promoting the uptake of research findings. , J Clin Epidemiol 58, 107-112.
- 16.NCM Theunissen, DTD deRidder, Bensing J M, GEHM Rutten. (2003) Manipulation of patient-provider interaction: discussing illness representations or action plans concerning adherence. , Patient Educ Couns 51, 247-258.
- 17.Aveyard P, Cheng K K, Almond J, Sherratt E, Lancashire R et al. (1999) Cluster randomised controlled trial of expert system based on the transtheoretical ("stages of change") model for smoking prevention and cessation in schools. , BMJ 319(7215), 948-53.
- 18.Michie S, Abraham C. (2004) Interventions to change health behaviours: Evidence-based or evidence-inspired?. , Psychol Health 19, 29-49.
- 19.Haynes R B, McDonald H, Garg A X, Montague P. (2002) Interventions for helping patients to follow prescriptions for medications. Cochrane Database Syst Rev(2):CD000011.
- 20.Sackett D L, Snow J C. (1979) The magnitude of adherence and non-adherence. In Compliance in Health Care. Edited by Haynes RB, Taylor DW, Sackett DL. Baltimore:JohnsHopkinsUniversityPress; 11-22.
- 21.Leventhal H, Cameron L. (1987) Behavioural theories and the problem of compliance. , Patient Educ Couns 10, 117-138.
- 23.Brawley L R, Culos-Reed S N. (2000) Studying adherence to therapeutic regimens: Overview, theories, recommendations. , Control Clin Trials 21, 156-163.
- 24.Dunbar J M, Marshall G D, Hovell M F. (1979) Behavioural strategies for improving compliance. In Compliance in health care. Edited by Haynes RB, Taylor DW, Sackett DL. Baltimore:JohnsHopkinsUniversityPress; 174-190.
- 25.Simoni J M, Pearson C R, Pantalone D W, Marks G, Crepaz N. (2006) Efficacy of interventions in improving highly active antiretroviral therapy adherence and HIV-1 RNA viral load: a meta-analytic review of randomized controlled trials. J Acquir Immune Defic Syndr43(Suppl 1):S23-S35.
- 26.Mannheimer S B, Morse E, Matts J P, Andrews L, Child C et al. (2006) Sustained benefit from a long-term antiretroviral adherence intervention: results of a large randomized clinical trial. J Acquir Immune Defic Syndr43(Suppl 1):S41-S47.
- 27.Griffin S J, Kinmonth A, MWM Veltman, Gillard S, Grant J et al. (2004) Effect on Health-Related Outcomes of Interventions to Alter the Interaction Between Patients and Practitioners: A Systematic Review of Trials. , Ann Fam Med 2, 595-608.
- 29.Rosenstock I M, Strecher V J, Becker M H. (1988) Social learning theory and the health belief model. , Health Educ Q 15, 175-183.
- 30.Rosenstock I M. (1990) The health belief model: Explaining health behavior through expectancies. In Health behaviour and health education. Edited by Glanz K, Lewis FM, Rimer BK. San Francisco: Josey-Bass;. 39-62.
- 32.Rogers R W. (1975) A protection motivation theory of fear appeals and attitude change. , J Psychol 91, 93-114.
- 33.Natrass N. (2012) The AIDS Conspiracy: Science Fights Back.New York:ColumbiaUniversityPress. 23-27.
- 34. (2014) Antiretroviral Pregnancy Registry Steering Committee.Antiretroviral Pregnancy Registry international interim report for1Jan1989–31July2014.Wilmington,NC:Registry Coordinating Center. Available at http://www.APRegistry.com.