
Delayed Laparoscopic Repair of Bladder Injury with Vesico Cutaneous Fistula in Fracture Pelvis
- Open Access
- Peer Reviewed
- Similarity Checked
- CC BY 4.0
Abstract
Small extra-peritoneal bladder injury is commonly treated conservatively as it heals spontaneously. However if there is an impinging bony spicule in the rent, the bladder wound does not heal and it is preferable to repair the rent primarily. We present a case of non healing extra-peritoneal bladder injury initially managed conservatively in a trauma center with supra-pubic catheter (SPC). Cystogram was done after 7 weeks showed persistent leakage of contrast. Hence patient was managed by laparoscopic repair of persistent extra-peritoneal bladder rent.
Article Information
- Received
- Accepted
- Published
Academic Editor: Ashwin Sridhar, University College London Hospital NHS trust, United Kingdom.
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2021 Senthil Kallappan
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Correspondence: A. K. M. Fazlul Karim, Department of Urology, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Urinary bladder lies deep in the bony pelvis, and hence it is protected from external trauma. Injury occurs due to motor vehicle collisions; following a fall; assaults blows to the lower abdomen and crush injuries. Extra peritoneal bladder injuries are more commonly associated with pelvic fractures and they usually present with hematuria. Disruption of the bony pelvis can result in extraperitoneal tear of the bladder and its fascial attachments. Bone fragments can directly lacerate the bladder1. Compared to intra peritoneal bladder injury, extra peritoneal bladder injury is confined. Computerized tomographic urography is the investigation of choice. Most of the extra peritoneal bladder injuries are managed conservatively. Occasionally surgical intervention might be required2.
Case History
17-year-old male was referred with a urethral and suprapubic catheter and complaints of fever and pyuria for 6 weeks. The prior record showed that he was admitted 2 months earlier following a road traffic accident with pain in the lower abdomen, hematuria and anal tear. He was initially stabilized and was evaluated with a CT scan which showed a pelvic fracture; extra-peritoneal bladder injury at two sites in the antero-lateral wall. The attending trauma surgeon did diverting colostomy for anal tear and supra-pubic cystostomy. Patient was referred after 6 weeks of fever and pyuria. Clinical examination revealed fair general condition and abdomen examination revealed a well-healed midline laparotomy scar along with colostomy, supra-pubic and urethral catheters. Bio-chemical investigation revealed normal renal function. Urine culture was positive and he was treated with culture specific antibiotic as he was symptomatic. After 7 days of treatment, computerized tomographic cystogram was done, which showed bilateral extra peritoneal bladder tears of about 15mm in length with extravasation of contrast from the anterolateral wall of bladder close to bladder neck bilaterally. Figure 1(A). Considering the persistence of gross extravasation of bladder contrast even after 7 weeks; laparoscopic repair of the bladder rent was planned.
Sigmoid colostomy was covered with sterile adhesive. With the patient in supine position, using 4 ports, laparoscopy was done. Figure 1 (B). There were extensive omental and bowel adhesions, which were released. Bladder was dropped and the SPC was removed. Extensive fibrosis was noted between the anterior wall of the bladder and pubic bone. Further mobilization of anterior wall of bladder revealed a bone spicule impinging on the left anterolateral wall and causing a rent of about 15 mm. The other rent was noticed on the right anterolateral wall close to the bladder neck about 15 mm long. Figure 1 (C). The bone spicule was removed.
Diluted methylene blue solution was instilled through urethral catheter to confirm that there were no other rents. The two rents were connected and made into a single large rent. Figure 1 (D). The edges were trimmed and closed using 3-0 absorbable barbed suture and omentum was tacked over the suture line.
Figure 1. A. Pre-operative CT showing contrast extravasation in anterior wall with bony spicule; B. Port Placement for bladder repair; C. Bladder rent identified by methylene blue; D. Two defects joined into a single cystotomy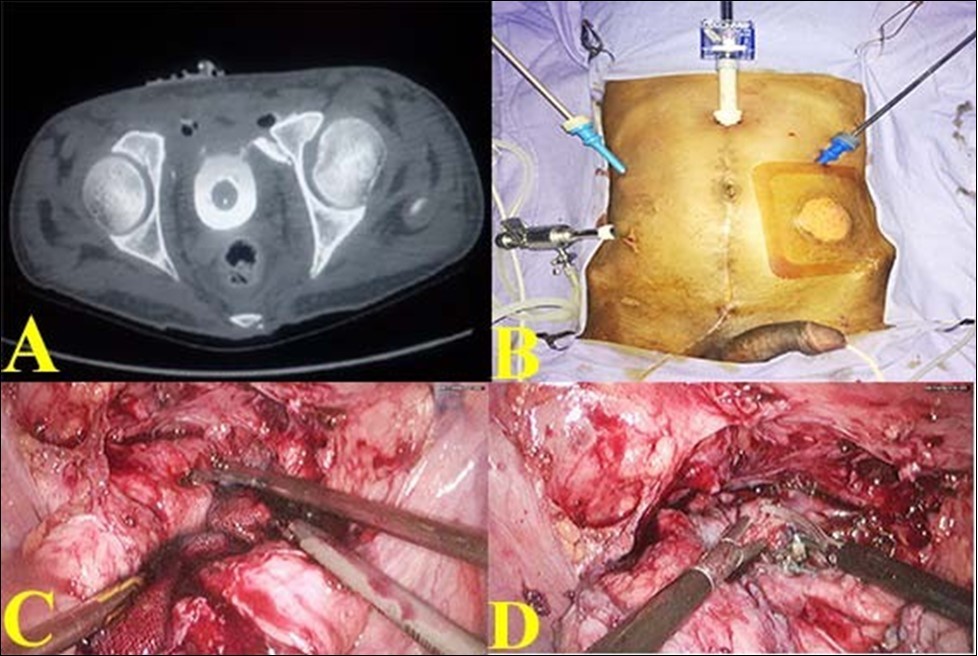
Download figure
(Figure 2 (G). SPC was reinserted. Bladder was again distended with dilute methylene blue solution to make sure that the closure was watertight. A tube drain was placed. Postoperatively patient made an uneventful recovery. Tube drain was removed on 7thpostoperative day when the drainage was less than 10ml. SPC was removed on the 10thpostoperative day. CT cystogram was done on 21st day which showed no extravasation Figure 2 (H). Patient voided freely on removal of urethral catheter on 21st day.
Figure 2. E. Bladder rent closing with barbed suture ; F. Suturing completed; G. Omental reinforcement over the suture line; H. Post operative CT showing healed bladder.
Download figure
Discussion
About 1.5% of patients having a blunt trauma to the abdomen can have bladder injuries. Bladder injury occurs in 6% of patients with pelvic fractures. Injury occurs due to road traffic accidents especially if the bladder is distended.
Bladder injury may or may not be associated with fracture of the pelvis1. Blunt trauma to the abdomen with a distended bladder causes rupture of the dome of the bladder into the peritoneal cavity as it is the weakest portion. (Intraperitoneal bladder rupture)
Gross hematuria is a common sign in bladder rupture. In a conscious patient, other symptoms like abdominal pain, supra-pubic discomfort and inability to urinate can be present. Computed tomography is the Investigation of choice to identify the extent of the bladder injury. It also helps in identifying other intra- abdominal injuries and pelvic fracture. Computed tomography has a sensitivity of 95 % in the diagnosis of bladder trauma. Gold standard investigation in diagnosis of bladder injury is retrograde cystogram or Computed tomographic cystogram2. Small extra peritoneal injuries are commonly managed by indwelling foley catheter for a period of 14 days. Small Isolated extraperitoneal bladder rupture can be managed conservatively with prolonged bladder drainage for about 3 weeks3. Operative repair is preferred if a impinging bony fragment from a pelvis fracture causes extra peritoneal bladder injury 2.
Indications for surgical repair in extra peritoneal bladder injury (Level of evidence 3):
1) Failure of the catheter to provide adequate drainage (clot formation, persistent extravasation).
2) Concomitant vaginal or rectal injury.
3) Bladder neck injury not allowing placement of urethral catheter.
4) Patients undergoing internal fixation of a pelvic fracture requires bladder repair to prevent urinary extravasation and infection of orthopedic hardware.
5) Patients undergoing laparotomy for other than urological injuries 3.
In the author’s case, patient presented 6 weeks post trauma. The patient had pyuria with significant extravasation. This is the first report of delayed laparoscopic repair of extra-peritoneal bladder injury.
Gregory J. Wirth and associates reported 22 cases of extra peritoneal bladder injury. 12 patients (55%) underwent suturing for bladder injury with a delay of 2.7 days. 2 patients were repaired due to fear of paravesical hematoma infection4.
Brad Figler and associates reported that in extra-peritoneal bladder injury; prolonged extravasation (15%) needed surgical intervention.
Conclusion
When compared to intra peritoneal bladder injury, extra peritoneal bladder injury can be treated conservatively because of its self-limiting nature. However when there is persistence of gross extravasation even after conservative treatment, surgical repair is mandatory. To our knowledge this is the first case report of delayed laparoscopic repair of extra-peritoneal bladder injury.
Laparoscopy is a feasible, safe and less morbid procedure even for a delayed presentation of extra peritoneal bladder injury.
References
- 1.Allen F Morey, FACS Daniel D Dugi MD. (2016) . Campbell-Walsh urology, eleventh edition, Elsevier, Inc 2513-2516.
- 2.Tiffany D Marchand, Rene Hugo Cuadra, BS Daniel J Ricchiuti. (2012) Laparoscopic Repair of a Traumatic Bladder Rupture. , JSLS 16, 155-158.
- 3.Reynaldo G Gomez, Ceballos Lily, Coburn† Michael, Jr Joseph N Corriere, Christopher M Dixon et al. (2004) Consensus statement on bladder injuries. , BJU international 94, 27-32.